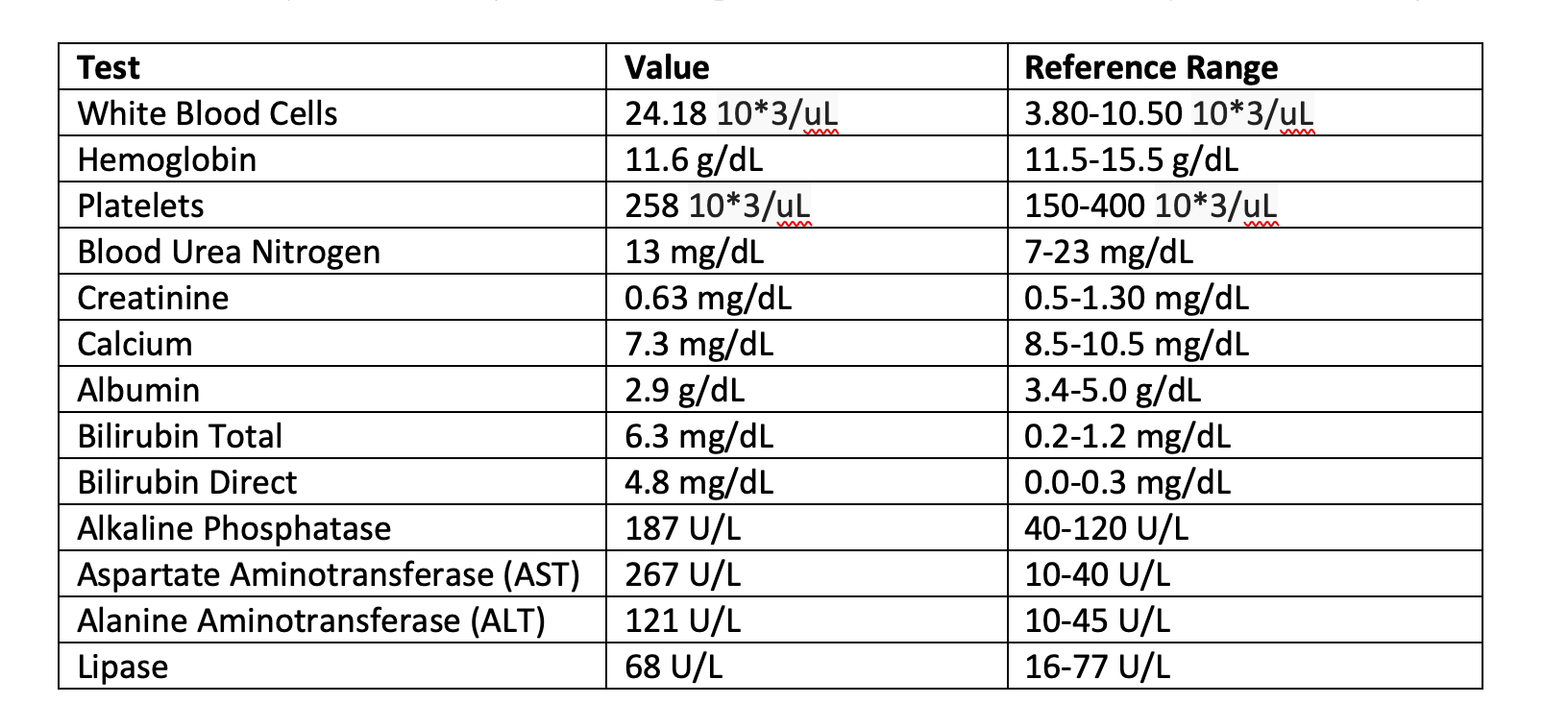
Case Presentation: 96 year old female with past medical history significant for hyperlipidemia and dementia who presented with altered mental status and hypoxia, admitted for acute hypoxic respiratory failure and septic shock. She denied fever, chills, nausea, vomiting, or weight loss. Laboratory evaluation revealed total bilirubin of 0.6 mg/dL, alkaline phosphatase of 184 U/L, and elevated AST 267 U/L and ALT 121 U/L. Abdominal ultrasound showed a dilated common bile duct measuring 14 mm, and a dilated fluid-filled gallbladder, with small gallstones but no masses. CT Abdomen and Pelvis demonstrated a substantially dilated gallbladder measuring 5.5 cm in cross-section and 16 cm in length. Small stones within the dependent gallbladder. Additionally, a 4.5 cm periampullary duodenal diverticulum was noted on imaging. Magnetic Resonance Cholangiopancreatography and Endoscopic retrograde cholangiopancreatography were discussed with the patient’s family; however they did not want any invasive diagnostic or therapeutic interventions even if they were life saving.
Discussion: Lemmel’s syndrome is a rare but important cause of obstructive jaundice, most often seen in older adults where periampullary diverticula are more prevalent. Although periampullary diverticula are commonly incidental, a small subset becomes symptomatic. Lemmel’s syndrome specifically refers to biliary obstruction caused by external compression of the distal common bile duct by a periampullary diverticula in the absence of stones, malignancy, or intrinsic biliary disease.Pathogenesis involves direct mechanical compression by a diverticulum or functional obstruction from inflammation-related fibrosis and impaired sphincter of Oddi motility. Chronic stasis may predispose patients to recurrent biliary symptoms or cholangitis. Clinically, patients present with jaundice, pale stools, dark urine, pruritus, and cholestatic liver enzyme elevation. The absence of abdominal pain can delay diagnosis. In our case, the lack of fever, leukocytosis, or abdominal tenderness reduced suspicion for pancreatitis or cholangitis.Imaging is essential but often limited. Ultrasound may show biliary dilation but poorly visualizes periampullary diverticula. MRCP provides noninvasive biliary assessment but may miss small diverticula. CT is more sensitive, particularly for air or contrast-filled diverticula, but its correlation with obstruction is indirect. ERCP remains the diagnostic gold standard, allowing direct visualization and immediate therapy. In this case, imaging identified a large diverticula compressing the distal CBD, however the family declined further interventions.The differential diagnosis of obstructive jaundice is broad, but in the absence of stones or masses, extrinsic compression by a diverticulum should be considered. Endoscopic treatment, sphincterotomy and/or stenting, is typically effective, while surgery is reserved for refractory cases. This case emphasizes the importance of recognizing Lemmel’s syndrome as a treatable cause of biliary obstruction.
Conclusions: Lemmel’s syndrome is a rare but treatable cause of biliary obstruction. Clinicians should maintain a high index of suspicion in patients with unexplained obstructive jaundice, particularly when imaging fails to identify stones or tumors. Recognition of periampullary diverticula and use of ERCP are essential for diagnosis and management. Timely intervention can prevent serious complications and improve patient outcomes.