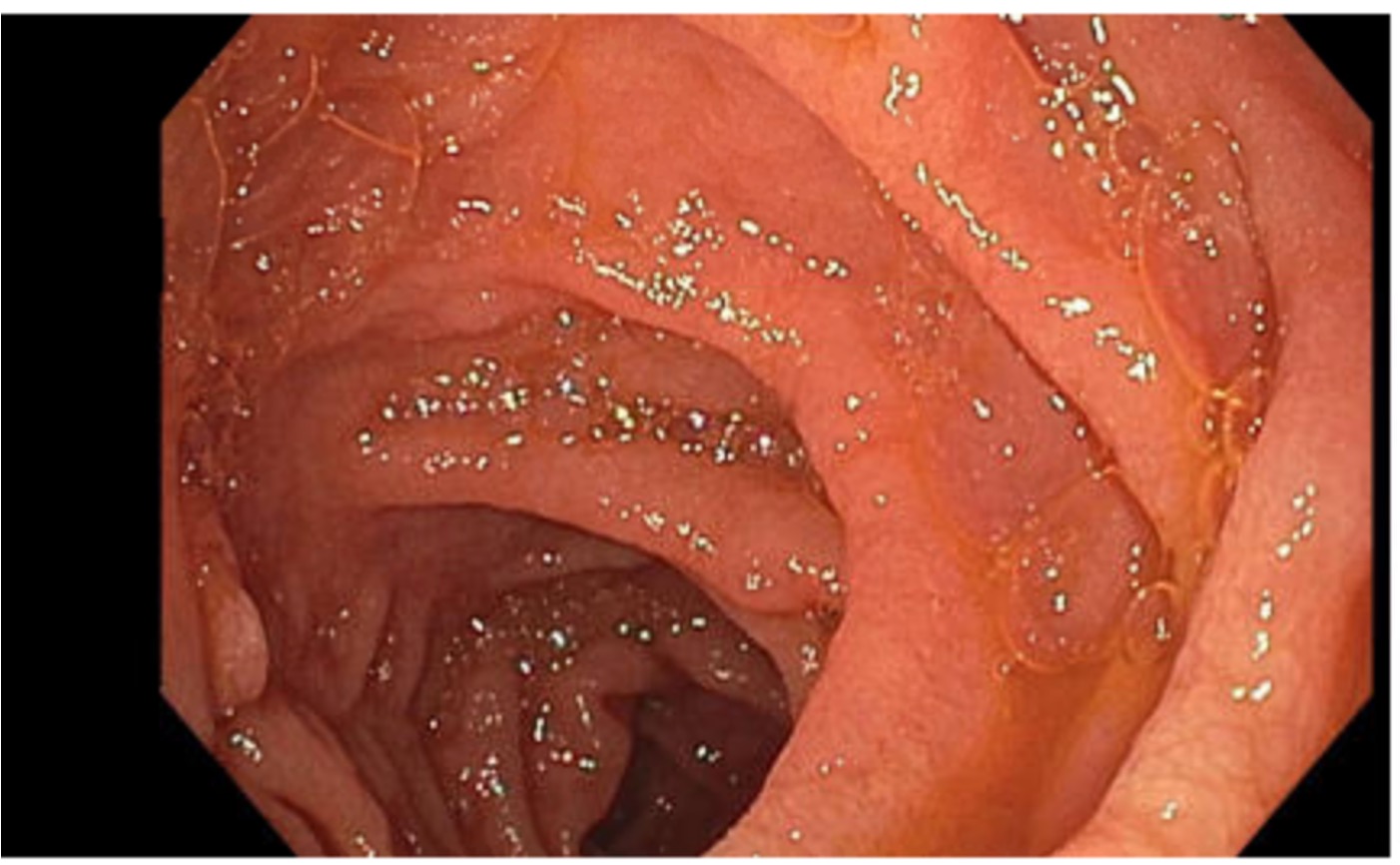
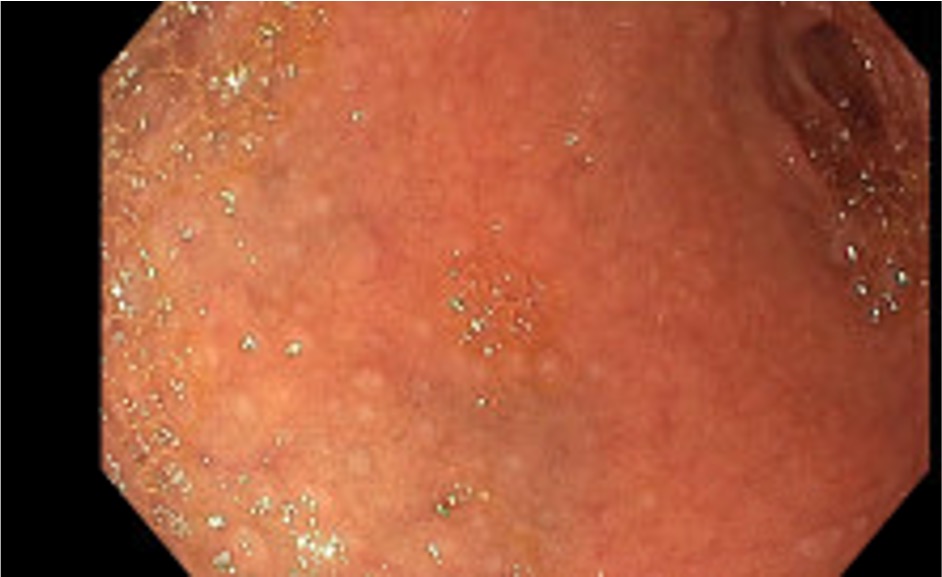
Case Presentation: Our patient was an 85 y/o female with a history of pulmonary embolism/deep venous thrombosis on warfarin, paroxysmal atrial fibrillation, and hypertension who presented to an outpatient gastroenterology (GI) appointment for evaluation of chronic diarrhea. She reported intractable, watery diarrhea for the past 9 weeks, with 3-4 stools/day as well as poor oral intake and a 50-pound weight loss. She denied recent travel, sick contacts, fevers, emesis, hematochezia, abdominal pain, changes in diet. Since the onset of diarrhea, her International Normalized Ratio (INR), which had previously been well-controlled, became persistently supratherapeutic, requiring multiple adjustments to her warfarin dosing. At her initial GI appointment, she was instructed to present to the Emergency Department for dyspnea and concern for an irregular heart rhythm on exam. On admission, she was afebrile with normal vitals and an unremarkable physical exam. Notable labs included white blood count 9.33 K/cumm, hemoglobin 12.9 gm/dL, chloride 114 mmol/L, bicarbonate 10 mmol/L, blood urea nitrogen 63 mg/dL, creatinine 2.7 mg/dL (baseline 1.2-1.4), INR 26.85, prothrombin time 267.3, and partial thromboplastin time 98. A gastrointestinal pathogen panel and cross-sectional imaging were negative. Fecal calprotectin was elevated at 1204. Esophagogastroduodenoscopy (EGD) and colonoscopy showed scalloped mucosa in the duodenum and nodular mucosa in the duodenal bulb concerning for Olmesartan-induced enteropathy (see Figures 1 and 2). Biopsies demonstrated acute erosive duodenitis, benign colonic mucosa, no evidence of microscopic colitis, and acute ileitis. Olmesartan was held on admission and the patient’s diarrhea improved. Her INR normalized with vitamin K supplementation and remained therapeutic with resumption of home warfarin dose. Olmesartan was discontinued on discharge, and she was scheduled for outpatient follow-up with GI and her warfarin clinic.
Discussion: Olmesartan-induced enteropathy is rare, first identified in 2012. Patients typically present with nausea, emesis, chronic diarrhea, and weight loss. EGD can demonstrate scalloping of the duodenal mucosa, similar to other sprue enteropathies, including Celiac disease. Often, though not always, biopsy demonstrates sprue-like histology within the intestines (villous atrophy, increased intraepithelial lymphocytes, and increased subepithelial collagen). Supratherapeutic INR has been known to occur in patients with diarrhea and decreased oral intake. In this case, the likely cause of the patient’s supratherapeutic INR was Olmesartan-induced enteropathy, which rapidly improved after withholding the medication. This case highlights the importance of a comprehensive medication review in the hospital and continued vigilance for adverse drug reactions.
Conclusions: Olmesartan-induced enteropathy is a rare cause of chronic diarrhea that can result in further complications, such as acute renal injury and supratherapeutic INR. Providers should conduct thorough reviews of medications in the hospital setting.