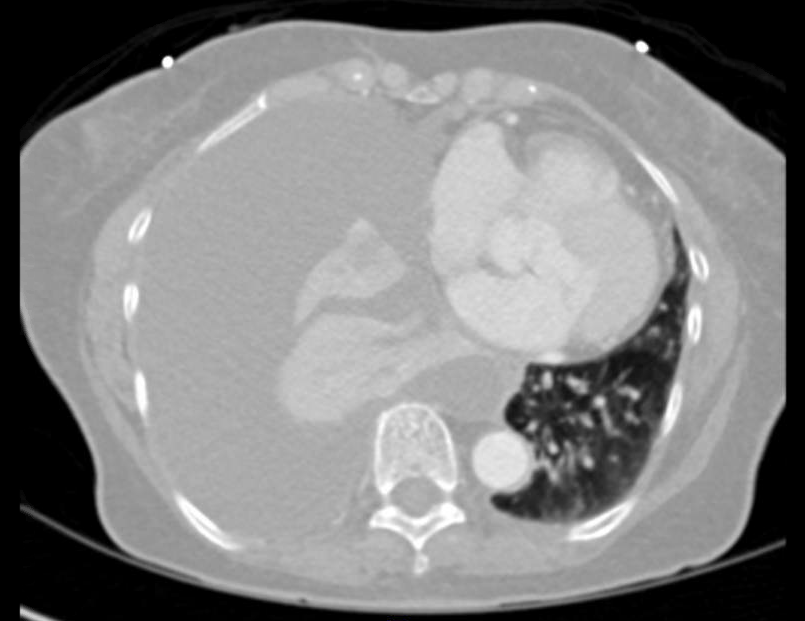
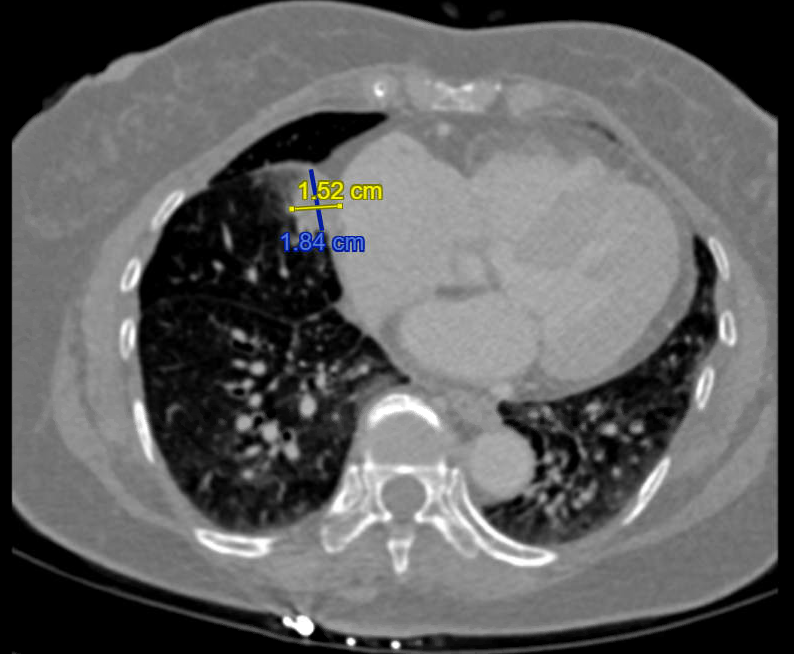
Case Presentation: A 56-year-old Vietnamese woman, lifetime nonsmoker, with papillary thyroid carcinoma treated definitively in 2008 (undetectable thyroglobulin since), presented with acute dyspnea, orthopnea, and unintentional weight loss over several months. Imaging revealed a large right pleural effusion coinciding with symptom onset; thoracentesis drained 1.5 L amber fluid. Cytology showed malignant cells positive for AE1/AE3, CK7, and TTF-1, initially raising concern for thyroid cancer recurrence versus lung adenocarcinoma. Recognizing potential anchoring, the team broadened the differential. Post-thoracentesis CT revealed enlarging right lung nodules. Expanded immunohistochemistry (Napsin A positivity) confirmed a new primary lung adenocarcinoma. Staging showed no brain metastases. She started carboplatin, pemetrexed, and pembrolizumab; molecular testing revealed PD-L1 expression and an EGFR mutation, prompting transition to Osimertinib. She remains on Osimertinib with unchanged neoplasm on recent CT.
Discussion: Evaluating pleural effusions in patients with remote malignancies are vulnerable to anchoring bias—prematurely attributing findings to prior cancer. Anchoring bias can delay recognition of second primary malignancies, particularly when immunohistochemical markers overlap. Papillary thyroid carcinoma (PTC) rarely recurs after more than 10 years, especially with persistently undetectable thyroglobulin; thus, anchoring on thyroid cancer recurrence risked delaying the correct diagnosis. Deliberate debiasing—challenging assumptions, broadening differentials, and coordinating imaging, IHC, and molecular testing—are essential for accurate diagnosis. Diagnostic panels for malignant pleural effusion should include multiple lineage markers when the primary site is uncertain, especially in patients with previous malignancies. With 10–15% of survivors developing second primary cancers within 10 years, physicians must maintain vigilance and leverage multidisciplinary teams. Post-thoracentesis CT imaging revealing enlarging pulmonary nodules demonstrates how large effusions can obscure underlying parenchymal disease. Repeat imaging after fluid drainage should be routine in unclear cases.
Conclusions: New abnormalities in patients with remote cancer histories should not be presumed to recurrence. Awareness of anchoring bias and structured diagnostic reasoning can identify second primary malignancies early, directly improving patient outcomes.