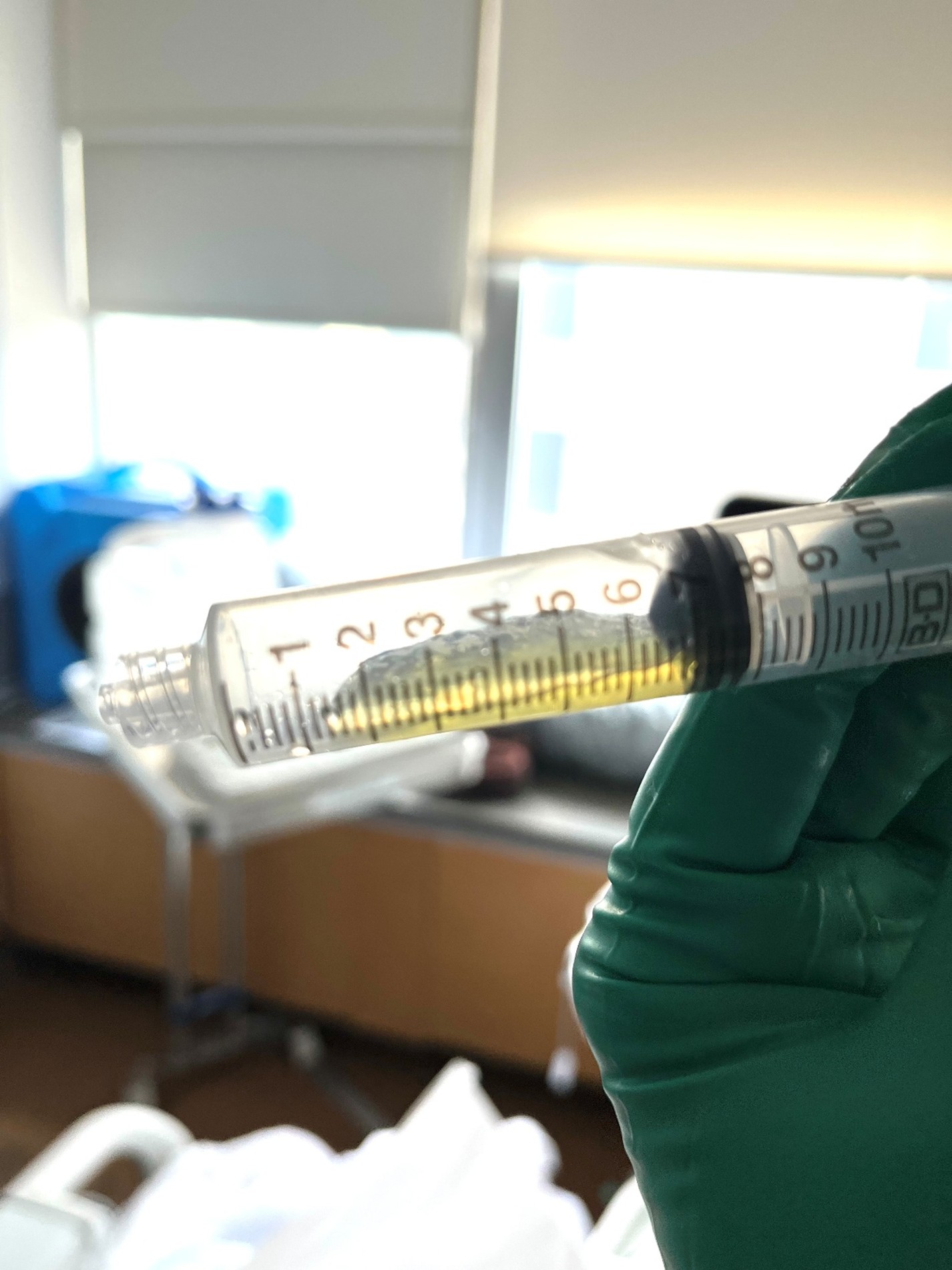
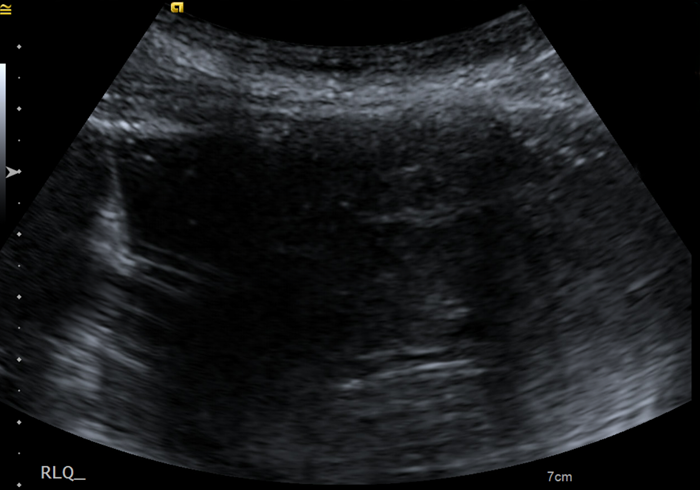
Case Presentation: A 70-year-old woman presented with 5 months of increasing abdominal distension. Her exam was notable for a markedly distended abdomen with dullness to percussion. CT imaging revealed large volume ascites with average Hounsfield Unit around 20, obscuring underlying structures. Bedside POCUS showed a large pocket of complex fluid that appeared safe for paracentesis. An 6 Fr catheter was inserted, and an initial flash of fluid was obtained. However, further aspiration was unsuccessful despite confirmation of correct catheter placement with an ultrasound. Upon close inspection, the aspirated fluid resembled straw-colored, viscous, gelatinous material raising concern for pseudomyxoma peritonei. Paracentesis was reattempted by Interventional Radiology, who was able to remove 1 L fluid using a larger 12 Fr catheter and vacuum suction.Cytology revealed abundant mucinous material consistent with a mucinous lesion but no presence of tumor cells. Her CEA level was elevated at 49 ng/mL but CA125 and CA 19-9 were normal. She underwent exploratory laparotomy with evacuation of 10 L of intra-abdominal mucin. Additionally, an appendectomy was performed for a firm nodularity on the appendix with mucinous deposits on the surface, a left oophorectomy for a large left ovarian mucinous lesion, and omentectomy with peritoneal stripping. Pathology was consistent with stage IV mucinous adenocarcinoma of appendiceal origin. Adjuvant FOLFOX was started with consideration to proceed with complete cytoreduction (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) in the future.
Discussion: Complex ascites with sonographic features such as increased echogenicity, septations, loculations, and debris are most often caused by infections, hemorrhage, malignancy, or inflammation. Mucinous ascites is extremely rare and seldom considered based on radiographic findings alone. CT imaging may provide clues such as a characteristic pattern of accumulation and higher densities. Acellular or paucicellular mucin pools with variable amounts of neoplastic mucinous epithelium are distinct features of pseudomyxoma peritonei, and negative cytology should not provide false relief.Mucinous appendiceal neoplasms are unique tumors characterized by abundant extracellular mucin comprising most of the tumor volume. They may present as distended mucin-filled appendix, or with peritoneal dissemination following rupture or transmural extension of the primary tumor. Peritoneal spread is characterized by significant intra-abdominal accumulation of mucinous ascites and tumor nodules referred to as pseudomyxoma peritonei. Many patients present with metastatic disease confined to the peritoneum. A combined therapeutic approach of CRS and HIPEC can offer favorable long-term outcomes.
Conclusions: 1. Failure to drain ascitic fluid despite correct technique should prompt reconsideration of the differential diagnosis rather than repeated bedside attempts. 2. Recognition of gelatinous fluid as a diagnostic clue is critical for early identification of mucinous malignancies, which can expedite oncologic evaluation and improve outcomes