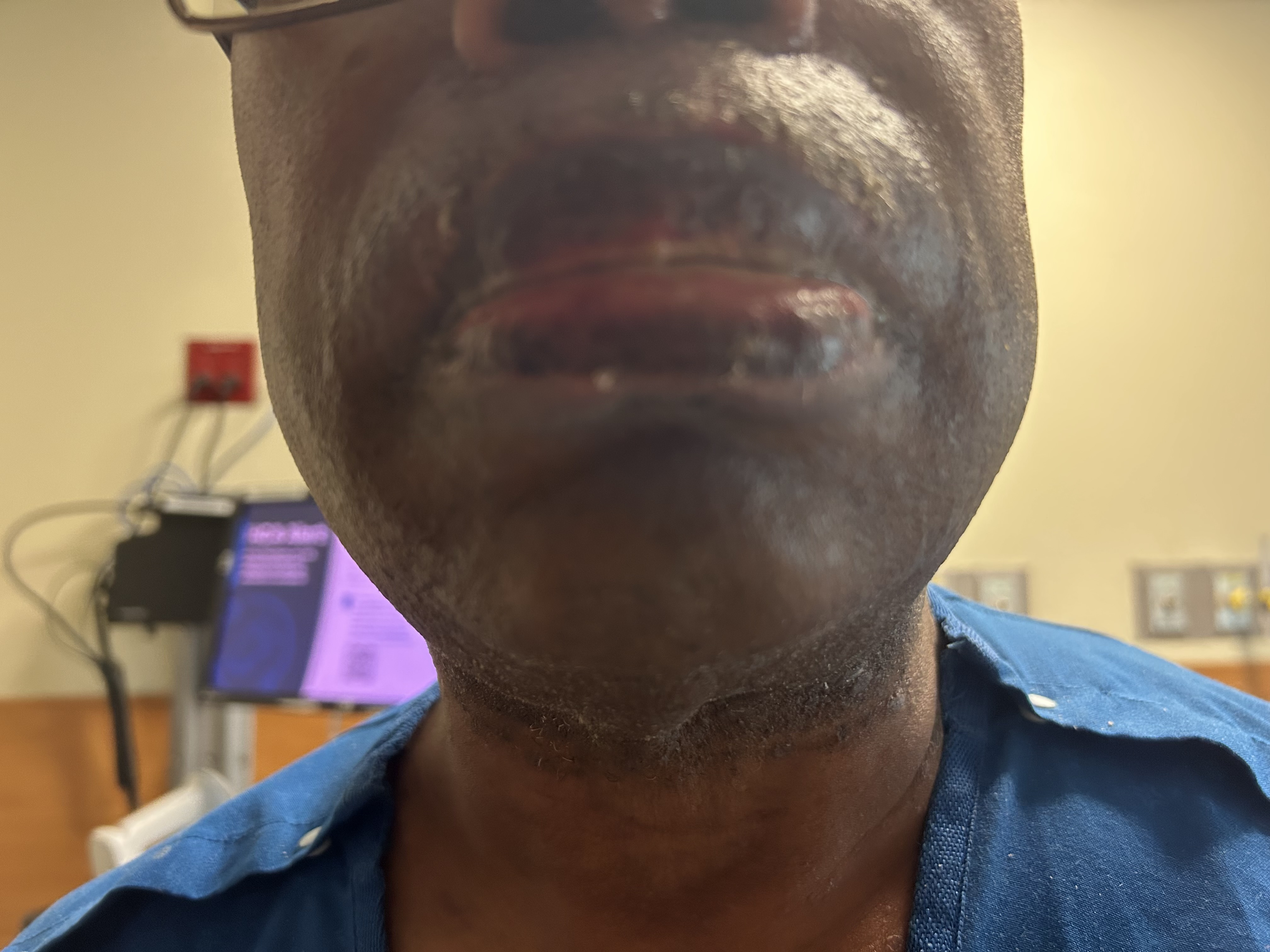
Case Presentation: A 59-year-old male with chronic lymphocytic leukemia (CLL), hypertension, and hyperlipidemia presented with painful oral ulcerations and a minor rash on back. Patient’s ulcers were mildly improved on oral fluconazole prescribed by his primary care provider. On admission, oral mucosa was erythematous, ulcerated, and had white plaques across the palate. A small hyperpigmented planar rash was present on the lower back and behind the right ear. WBC was 42,000/uL; all other labs were unremarkable. Direct laryngoscopy with biopsy revealed diffuse white plaques and ulcerations on the larynx and pharyngeal walls. He was diagnosed with oral versus oral-esophageal candidiasis and switched to IV micafungin from oral fluconazole given his history of CLL. Soft palate biopsy showed acute inflammatory exudates and ulcer debris. Symptoms improved, and patient was discharged on 21-day course of oral fluconazole, given stable counts and low suspicion of sepsis. He returned five days later with severe oral blistering, lip swelling, and extensive pruritic rash involving arms, back, and groin. Fluconazole-induced allergic reaction was suspected with concern for evolving Stevens-Johnson syndrome (SJS) prompting discontinuation of fluconazole and initiation of IV methylprednisolone and oral diphenhydramine. IV micafungin was started to resume anti-fungal treatment. Patient’s lip swelling and ulcerations improved and was discharged on prednisone, diphenhydramine, and outpatient IV micafungin. Patient returned to the hospital 5 days later with worsening of his prior rash. Severe oral mucosal blisters and ulcers were noticed with lip swelling. The rash on the back was now scaly, thickened and intensely pruritic, extending across the trunk and arms. Allergic reaction to IV micafungin was suspected prompting its cessation and initiation of IV methylprednisolone and diphenhydramine. Punch biopsy of the lower back was done, which later came back positive for lichen planus. Patient’s rash and lip swelling improved substantially and was discharged on high dose prednisone taper regimen. Outpatient dermatology follow up was also recommended.
Discussion: This case highlights the diagnostic complexity of distinguishing drug hypersensitivity from autoimmune conditions in immunocompromised patients. Firstly, the temporal occurrence of rash after initiation of anti-fungals and its improvement after steroids strongly suggest an allergic component. But the biopsy-proven lichen planus complicates the picture. Oral lichen planus can manifest as while plaques and ulcerations making it a key differential for the initial oral lesions. Secondly, improvement of the symptoms with steroids is consistent with treatment of both drug hypersensitivity and severe lichen planus. Ultimately, the pathologic diagnosis of lichen planus provides the highest level of diagnostic certainty. It is questionable whether this was simply a coincidental flare of lichen planus due to candidiasis in a CLL patient, a drug-induced lichenoid eruption mimicking lichen planus, or misdiagnosis of SJS that was a fulminant lichen planus/drug-induced lichenoid eruption.
Conclusions: Clinicians should consider broad differentials in immunocompromised patients presenting with severe mucocutaneous eruptions. Early dermatology consultation and prompt biopsy are crucial for accurate diagnosis, minimizing inappropriate management, and improving patient outcomes.