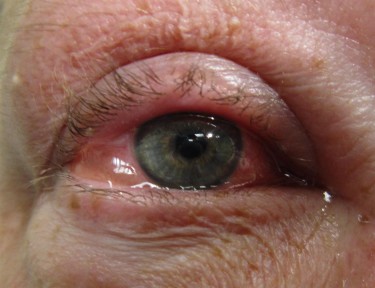
Case Presentation: A 72-year-old male with a past medical history of hypertension and hyperlipidemia presented with progressive left-sided facial pain involving the cheek, jaw, and ear, worsened by arm elevation. Over two weeks, he developed worsening headache, fever up to 39.2°C, and periorbital swelling. He had recently completed antibiotics for a dental infection. On admission, he reported diplopia and photophobia.On examination, he was febrile (39°C), with otherwise stable vital signs. Neurologic findings included left-sided ptosis, complete ophthalmoplegia involving cranial nerves III, IV, and VI, reduced corneal reflex (CN V1), and papilledema. The left eye was erythematous, edematous, and had purulent discharge.Laboratory tests revealed leukocytosis (WBC 34,300/mm³, neutrophilic predominance). Blood cultures were negative, but an abscess culture later grew coagulase-negative Staphylococcus, Actinomyces meyeri, and Streptococcus viridans.MRI with contrast confirmed left cavernous sinus thrombosis (CST) with adjacent inflammation. CT of the neck showed left subcutaneous facial edema and parotid gland enlargement. Venous ultrasound revealed absent flow in the left cavernous sinus.The diagnosis of septic CST secondary to a facial abscess was made. The patient was started on empiric IV vancomycin and piperacillin-tazobactam, and later transitioned to IV amoxicillin based on culture results. After ruling out contraindications, therapeutic anticoagulation with low molecular weight heparin was initiated. Supportive care included antipyretics, IV fluids, and close neurological monitoring.The patient improved significantly within 72 hours, with defervescence and gradual recovery of ocular function. He completed four weeks of IV antibiotics and a three-month course of anticoagulation.
Discussion: Cavernous sinus thrombosis is a rare but critical condition, often resulting from infections in the facial “danger triangle.” Infections from the midface can spread to the cavernous sinus via valveless facial and ophthalmic veins, leading to septic thrombosis.Typical features include fever, headache, periorbital edema, and cranial nerve involvement—particularly III, IV, V1, and VI—manifesting as ophthalmoplegia, ptosis, and sensory loss. In this case, the constellation of ocular and cranial nerve deficits strongly suggested CST.MRI with contrast and MR venography are the preferred diagnostic tools, allowing early visualization of thrombosis. While blood cultures may be negative, source cultures (e.g., abscesses) can guide therapy.Management hinges on early, broad-spectrum IV antibiotics targeting likely pathogens, including Staphylococcus, Streptococcus, and anaerobes. Our patient’s polymicrobial infection underscores the need for comprehensive coverage and culture-directed therapy.The role of anticoagulation remains controversial, but many clinicians use it to reduce thrombus propagation and improve venous drainage, provided there are no contraindications. In this case, anticoagulation was associated with a favorable neurological outcome.
Conclusions: This case emphasizes the importance of early recognition of CST in patients presenting with facial infections and neurological deficits. Rapid imaging, timely administration of broad-spectrum antibiotics, and judicious use of anticoagulation can be life-saving. Awareness of this rare but severe condition is crucial for reducing complications such as vision loss, stroke, and death.