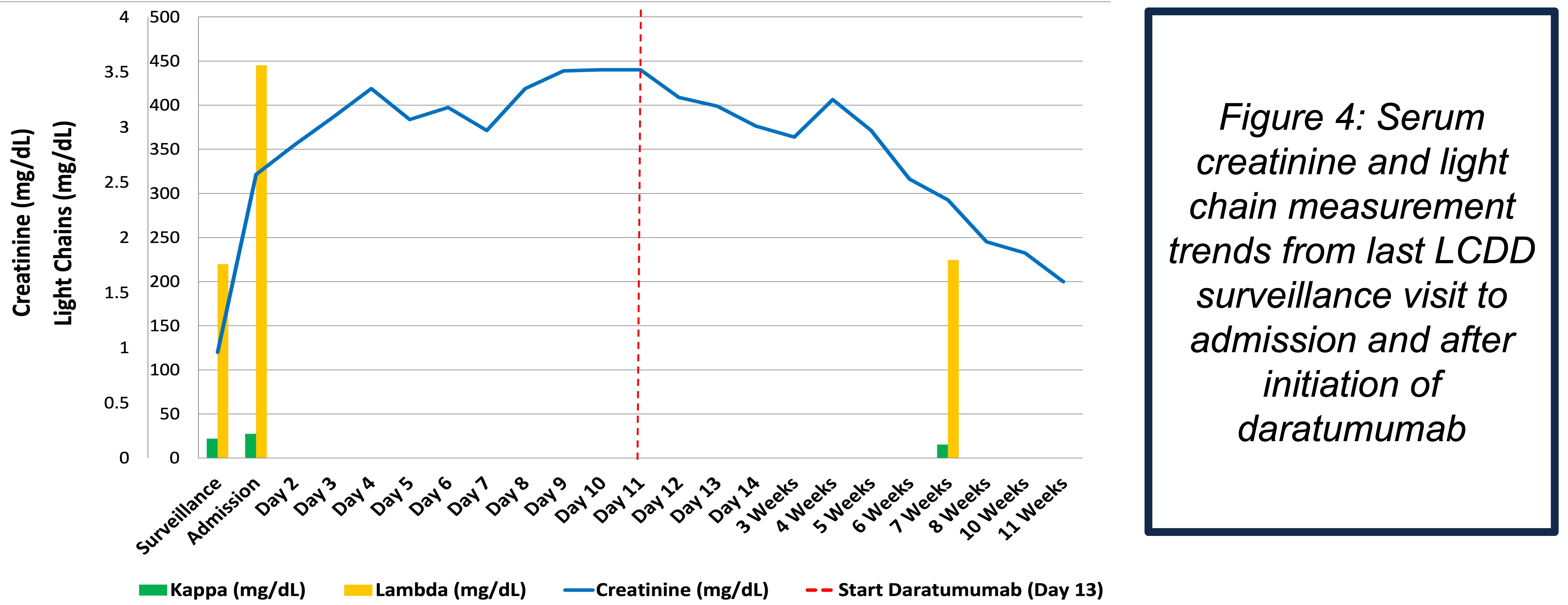
Case Presentation: An 83-year-old woman with HFpEF, atrial fibrillation on warfarin, chronic lymphocytic leukemia, hypertension, hypothyroidism, and a history of light chain deposition disease (LCDD) presented with 10 days of worsening dyspnea on exertion, orthopnea, and leg edema. Blood pressure on arrival was 219/107 mmHg. Exam showed mild respiratory distress, bibasilar crackles, and pitting edema to the knees. Labs revealed WBC 15.4 K/mm³, hemoglobin 9.9 g/dL, bicarbonate 20 mmol/L, BUN 49 mg/dL, and creatinine 2.5 mg/dL (baseline 0.9). BNPP was 8,419 pg/mL. Urinalysis showed 3+ protein, pyuria, and hematuria. Urine protein was 7.9 g/day, and urine immunofixation detected a monoclonal lambda light chain.Chest radiography showed cardiomegaly with pleural effusions. Renal ultrasound showed no obstruction. Echocardiogram demonstrated preserved LVEF of 63%, unchanged from prior. Despite diuresis, antihypertensive therapy, and treatment of a concurrent Enterobacter UTI, renal function worsened.Renal biopsy revealed recurrent LCDD with linear lambda staining of basement membranes, granular electron-dense deposits, 80% podocyte foot process effacement, arterionephrosclerosis, focal eosinophilic tubulointerstitial nephritis, acute tubular injury, and 41% global glomerulosclerosis. Hematology initiated daratumumab and dexamethasone. Her creatinine peaked at 3.5 mg/dL, then improved to 1.6 mg/dL. Lambda free light chains decreased by more than 50% from 445 to 224 mg/L at two-month follow-up.
Discussion: Light chain deposition disease is a rare cause of acute kidney injury that often masquerades as far more common inpatient problems such as hypertensive nephrosclerosis, cardiorenal syndrome, or infection. This overlap frequently leads to diagnostic anchoring, particularly in older adults with multiple comorbidities. Hospitalists rarely encounter LCDD, but they frequently care for patients with renal dysfunction, making early recognition key to preserving renal function.In this case, recurrent LCDD that occurred several years after quiescence was the true driver of kidney injury. Her presentation could easily be attributed to hypertensive emergency or volume overload, but the degree of proteinuria, history of monoclonal disease, and lack of improvement with standard inpatient management prompted renal biopsy. Early identification re-directed care from supportive treatment toward clone-directed therapy. Daratumumab-based regimens have rapidly become central in managing plasma cell disorders causing renal injury. Timely initiation in this case stabilized kidney function and reduced light chain burden.This case emphasizes the importance of resisting anchoring bias and maintaining suspicion for LCDD in patients with heavy proteinuria or known monoclonal gammopathy.
Conclusions: Hospitalists should consider recurrent light chain deposition disease in patients with acute kidney injury, significant proteinuria, and a history of monoclonal gammopathy, especially when renal function does not improve with standard inpatient therapy. Renal biopsy remains essential for diagnosis and guides timely hematology-directed treatment. Early clone-targeted therapy can meaningfully alter kidney outcomes and prevent irreversible renal injury.
.jpg)