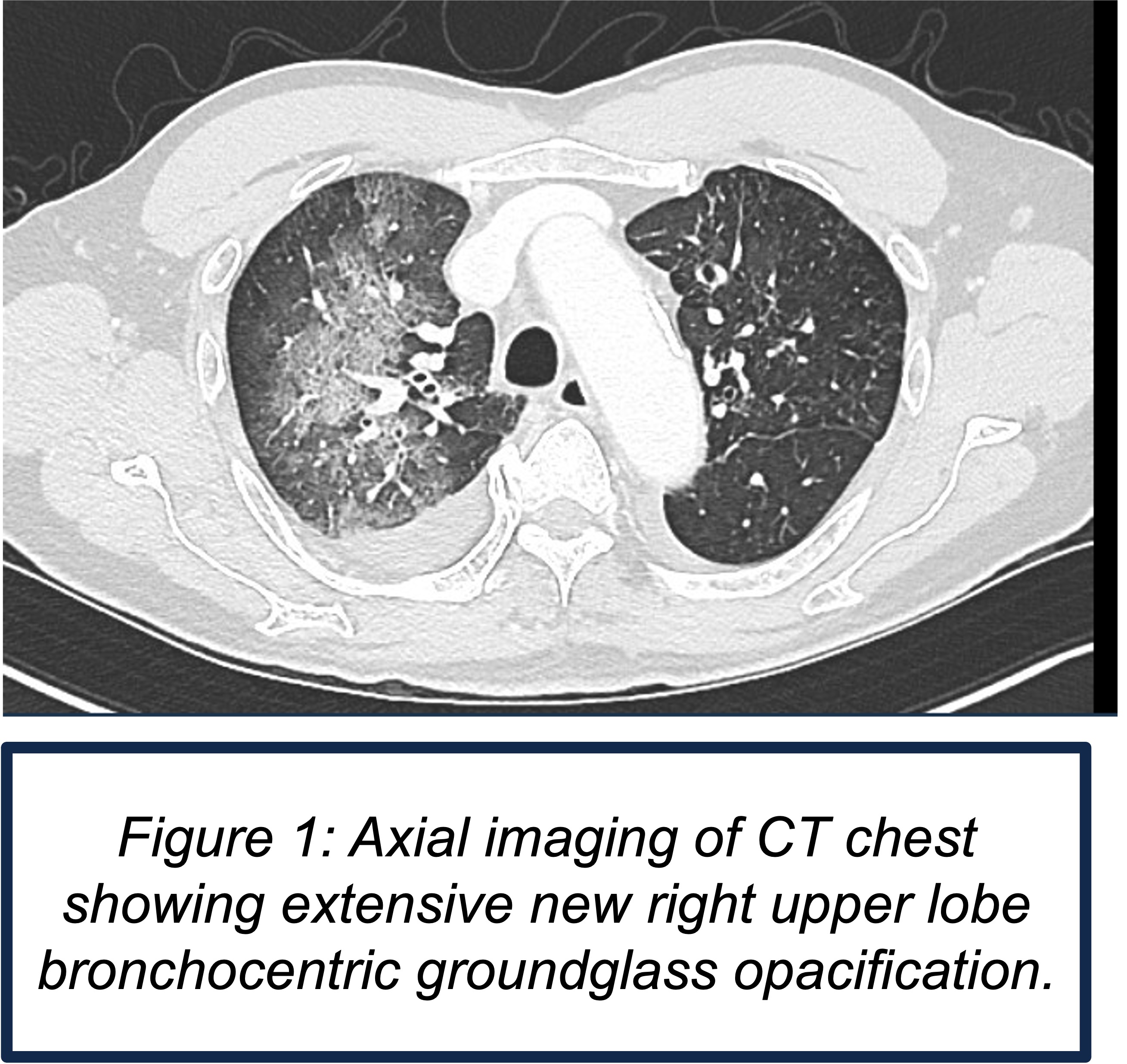
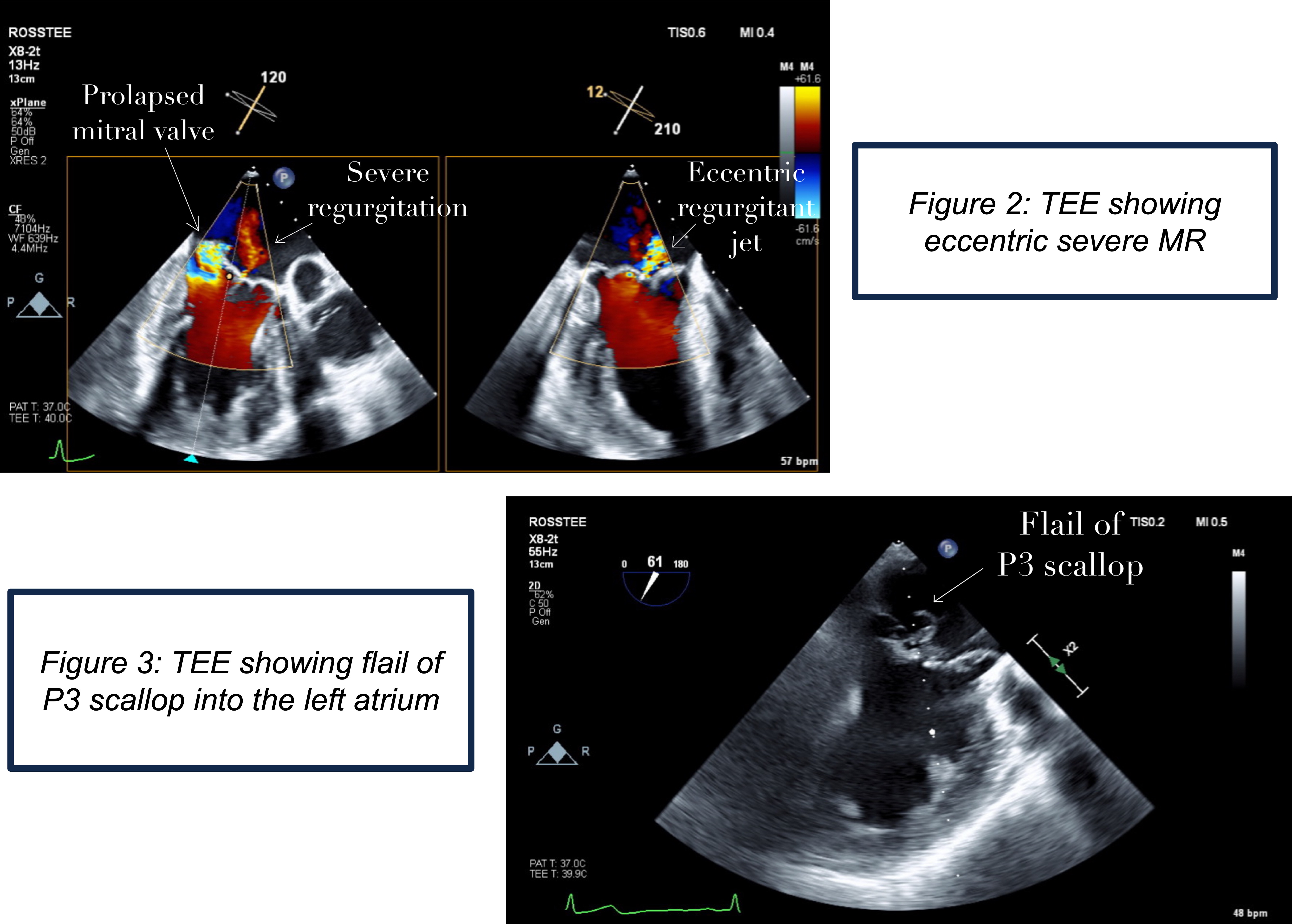
Case Presentation: An 80-year-old man with suspected latent tuberculosis, smoldering myeloma, and prior pulmonary embolism presented with four days of productive cough with blood-streaked sputum and two weeks of dyspnea on exertion. On arrival, he was afebrile, tachycardic up to 120 bpm, normotensive at 135/80 mmHg, and oxygenating at 95% on room air. Examination revealed a new grade 2/6 holosystolic murmur at the apex. Labs showed hemoglobin 12.5 g/dL, WBC 6.2 K/mm³, platelets 160 K/mm³, INR 1.2, troponin 22 ng/L, and BNP 159 pg/mL.Computed tomography of the chest demonstrated interstitial edema, small bilateral pleural effusions, and extensive bronchocentric ground-glass opacities in the right upper and lower lobes. A ventilation-perfusion scan showed no evidence of pulmonary embolism. Serial AFB smears, MTB PCR, and sputum cultures were negative. Empiric antibiotics for pneumonia were initiated.Transthoracic echocardiography revealed preserved LVEF (61%) and signs of acute severe mitral regurgitation (MR), including pulmonary vein systolic flow reversal, indicating an abrupt rise in left atrial pressure. Left atrial enlargement and moderate diastolic dysfunction simultaneously suggested chronic underlying MR. Pulmonology and cardiology determined that hemoptysis was most consistent with pulmonary venous hypertension secondary to acute severe MR. Transesophageal echocardiography identified the mechanism: flail of the P3 scallop with prolapse of the P2 scallop of the posterior mitral leaflet with chordal rupture, resulting in an eccentric severe mitral regurgitation.Hemoptysis resolved spontaneously. He was discharged with close follow-up and referral for mitral intervention.
Discussion: Hemoptysis is an uncommon but clinically important manifestation of acute severe mitral regurgitation. Sudden elevation in left atrial pressure leads to retrograde transmission into pulmonary veins, causing capillary rupture and alveolar hemorrhage. In this patient, chordal rupture produced flail P3 and P2 prolapse generated an eccentric jet toward the right pulmonary veins, explaining the right-sided ground-glass opacities. This is typical of primary degenerative MR. While infection, pulmonary embolism, and tuberculosis were initially considered, physical exam findings redirected the diagnostic pathway. The new apical holosystolic murmur challenged the presumed infectious etiology and ultimately led to the identification of acute valvular pathology. This case underscores the ongoing relevance of bedside examination in an era increasingly reliant on advanced imaging.
Conclusions: Acute severe mitral regurgitation should be considered in patients presenting with hemoptysis. Recognition of a new murmur can provide a critical diagnostic clue and prevent anchoring on more common pulmonary diagnoses. Early identification of acute valvular disease facilitates appropriate cardiology evaluation and timely referral for mitral intervention.