Background: Patients with impaired renal function are at an increased risk for adverse drug events (ADE) due to challenges in medication selection and dose adjustment. Morphine, while frequently used for rapid analgesia in the acute setting, poses a distinct risk in patients with an estimated glomerular filtration rate (eGFR) < 30 mL/min, as its active metabolites can accumulate and cause central nervous system and respiratory depression, as well as neurotoxicity. At our institution, two consecutive morphine-related ADEs in patients with impaired renal function underscored the imperative for a sustainable safety intervention beyond education alone.
Purpose: To reduce inappropriate morphine use in admitted patients with an eGFR < 30 mL/min through implementation of an IT-based system-level safety intervention that guides clinicians away from high-risk prescribing.
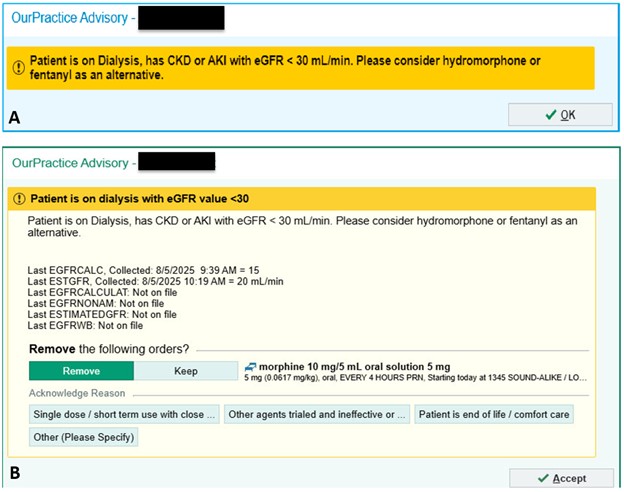
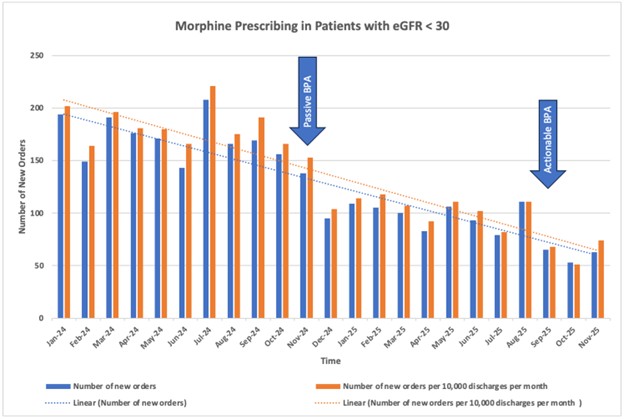
Description: We conducted a retrospective review of morphine orders placed in adult inpatients with an eGFR < 30 mL/min across five hospitals within our health system from January to October 2024. During this baseline period, an average of 172.3 inappropriate morphine orders were placed per month (184.2 orders per month per 10,000 discharges when adjusted for discharge volume). In response, a collaborative effort between hospital medicine, pharmacy, and IT led to the development of a best practice advisory (BPA) alert. This initial BPA was a passive alert triggered whenever morphine was ordered for patients with an eGFR < 30 mL/min, reminding prescribers of renal impairment and recommending alternative opioids with lower renal clearance, such as fentanyl or hydromorphone.From implementation in November 2024 through August 2025, the BPA reduced inappropriate morphine orders to 101.9 per month (109.4 per month when discharge-adjusted), representing a 41% decrease. Although effective, frequent bypasses still limited the BPA’s full impact, prompting revision to an actionable alert with a soft stop requiring prescribers to either cancel the order or to acknowledge and provide a justification for proceeding. Acknowledgment options included single dose with close monitoring, intolerance or failure of alternatives, patient on comfort care, and “other,” with a mandatory free-text explanation. Since implementation of the actionable BPA in September 2025, inappropriate morphine orders have decreased to an average of 59 orders per month (59.5 discharged-adjusted), representing an additional 42% reduction and a total decrease of 66% from baseline. Preliminary analysis revealed that 48.3% of triggered BPAs were bypassed, with 75.2% citing single dose with close monitoring, 4.0% intolerance or failure of alternatives, 10.9% comfort care, and 9.9% selecting “other” as reasons for override.
Conclusions: Implementation of a passive BPA reduced inappropriate morphine orders in patients with severe renal impairment. Converting the BPA to an actionable alert further enhanced its effectiveness, resulting in a substantial decrease in morphine orders to less than half of the baseline. Next steps include ongoing review of override patterns and evaluation of associated changes in adverse clinical outcomes. As we continue to monitor ordering and alert trends to fine tune our BPA, we anticipate that this intervention may foster sustained prescribing behavior change across all sites within our health system.