Background: Undercoding during billing is a widespread and costly problem among hospitalists. Undercoding is often driven by insufficient training and overreliance on complex medical decision-making (MDM) criteria. At our institution, internal benchmarking and comparison to national evaluation and management coding distributions revealed substantial undercoding across our hospitalist group. The 2023 Center for Medicare and Medicaid Services evaluation and management guideline changes (particularly the expansion and clarification of time-based coding) created an opportunity to reduce ambiguity, and improve coding accuracy through targeted education.
Purpose: To develop and implement a scalable, hospitalist-focused coding education initiative aimed at improving coding confidence and accuracy. We also aimed to reduce undercoding by increasing the utilization of time-based coding. Finally, we wanted to educate on proper use of critical care coding, and increase familiarity with the new extended care code.
Description: A multidisciplinary team consisting of a physician coding champion, an administrator, and coding specialists designed a streamlined education program centered around the 2023 CMS guideline updates. Curriculum content was intentionally simplified: individual CPT codes were distilled into single-slide summaries outlining indications and documentation requirements, including precise time thresholds.Interactive, case-based sessions were delivered to all hospitalists, with a coding specialist present for real-time clarification. Vetted dot phrases were provided for integration into the EHR. Recordings and written materials were shared broadly, and follow-up support was available via email, digital messaging, and in-person guidance.The program expanded to include dedicated sessions on extended care and critical care codes. An onboarding curriculum for new hires, targeted remediation for clinicians with outlier patterns, and an ongoing review of internal audits and RVU data to reinforce improvement and prevent regression was also implementedImplementation challenges included limited high-quality educational resources, resistance to change among experienced clinicians, complex real-world coding scenarios, and misaligned RVU attribution for shared-care situations. These were addressed through collaborative problem-solving with coding experts and continued updates to educational presentations.
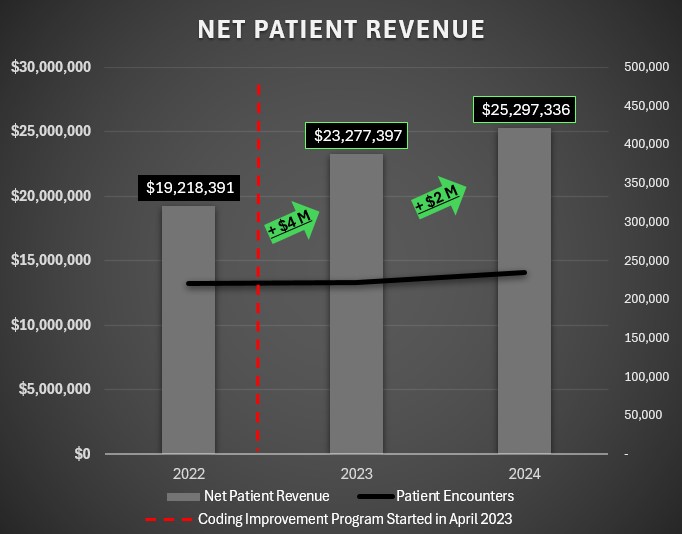
Conclusions: Based on internal audits, our interventions improved coding accuracy from 51% to 93%. Over a one-year period, the program increased annual collections by approximately $4 million without changes in the practice’s patient volumes. An engaging, active learning curriculum that utilizes and combines the interprofessional skills of coding specialists and administrative leadership with the clinical lens provided by a physician proved highly effective. We demonstrate that even entrenched coding habits can be successfully reshaped. This innovation offers a practical, scalable framework for other hospitalist groups seeking to improve accuracy and reclaim significant lost revenue.
.jpg)