Background: Effective interprofessional communication and agreement on patient care plans between providers and registered nurses (RNs) are fundamental to care delivery. Team-based models, such as regionalization in hospital medicine, aim to enhance collaboration by fostering relationships and increasing daily communication. Existing studies on regionalized care provide mixed results. This study aimed to evaluate whether regionalized hospitalist teams are associated with a higher level of interprofessional agreement on patient care plans.
Methods: We conducted a cross-sectional study of provider-RN dyads providing care in 12 general medical units at a tertiary academic medical center. Providers (physicians or APPs) were classified as regionalized if they cared for patients geographically regionalized to one inpatient floor, whereas non-regionalized providers cared for patients across multiple floors. A member of the study team collected data via in-person paper survey asking 4 questions on aspects of patient’s care plan for that day, including: (1) the primary diagnosis (2) scheduled tests or procedures for the day (3) patient’s top concern (4) estimated length of stay. The primary outcome was a composite total agreement score (0-8 points) derived from these questions. The survey also contained 3 questions on communication methods and frequency. Ordinal logistic regression modeled the relationship between regionalization and agreement, adjusting for provider and RN gender and years of experience. Secondarily, we evaluated individual- and dyad-level predictors of total agreement score.
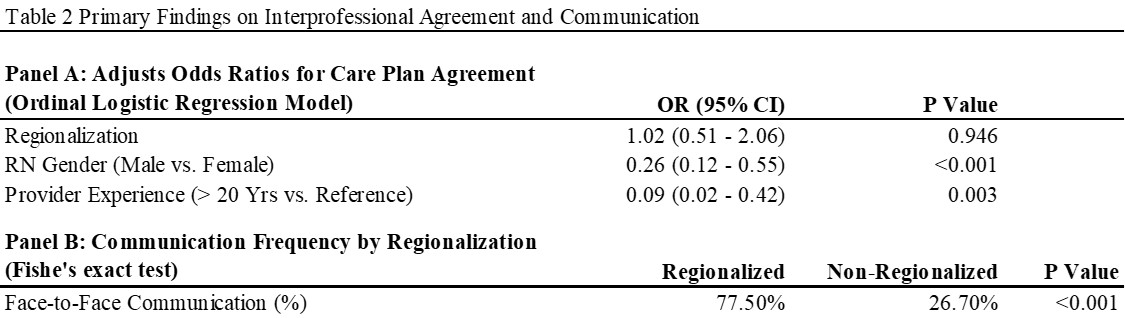
Results: We enrolled 203 provider-RN dyads resulting in 406 complete surveys. Survey respondent demographics were comparable across regionalized and non-regionalized teams (table 1). Regionalized teams had a significantly higher frequency of face-to-face communication (77.5%) compared to non-regionalized teams (26.7%, p< 0.001) although no statistically significant differences were observed between regionalized and non-regionalized teams on total agreement score (OR=1.02, 95% CI: 0.51-2.06, p=0.946) (table 2). There was also no difference between groups for each separate agreement element. Secondary analyses demonstrated male RNs had 74% lower odds of being in a higher agreement category than female RNs (OR = 0.26, 95% CI: 0.12-0.55, p < 0.001). Additionally, providers with 20 or more years of experience (OR=0.09, 95% CI: 0.02-0.42, p=0.003) had significantly lower odds of agreement compared to providers with less experience.
Conclusions: We found no significant association between team regionalization and provider-RN agreement, despite observed increase in face-to-face communication. This null result, consistent with prior research, highlights that team structure or face-to-face communication alone is insufficient to drive interprofessional agreement on care plans. Instead, effective communication pathways (even those structurally in place, such as multidisciplinary rounds) may require explicit reinforcement, standardization, or the integration of tools to ensure communication is not only present but effective. The significant influence of RN gender and provider experience on agreement suggests that individual communication styles play a critical role, further supporting the need for formalized structure. Future research should focus on implementing and testing these enhanced, standardized communication processes.
.jpg)