Background: Children often have small, poorly visible, or palpable veins, and are moving targets during peripheral intravenous catheter attempts. Landmark-based techniques are less than 50% successful, with further attempts leading to increased pain, anxiety, and delayed treatment. Baseline evaluation and our prior SHM poster identified high numbers of attempts, inconsistent escalation, and frequent cross-unit support. A multidisciplinary SPS Learning Team launched a quality improvement (QI) initiative to standardize Difficult IV Access (DIVA) scoring, escalation, and ultrasound use.
Methods: Baseline data (Apr–May 2024) were collected across all pediatric units using a paper bedside tracker capturing age, unit, number of attempts, and success. A pediatric IV guideline incorporating DIVA scoring, escalation steps, comfort measures, and ultrasound use was developed. Nurses and residents received ultrasound training. Pre/post pilot data (Jan–Oct 2025) included unit-level patient counts, IV attempts, and mean sticks per patient. Descriptive statistics and weekly run-chart review assessed trends. Process measures included DIVA documentation, algorithm adherence, and ultrasound utilization.
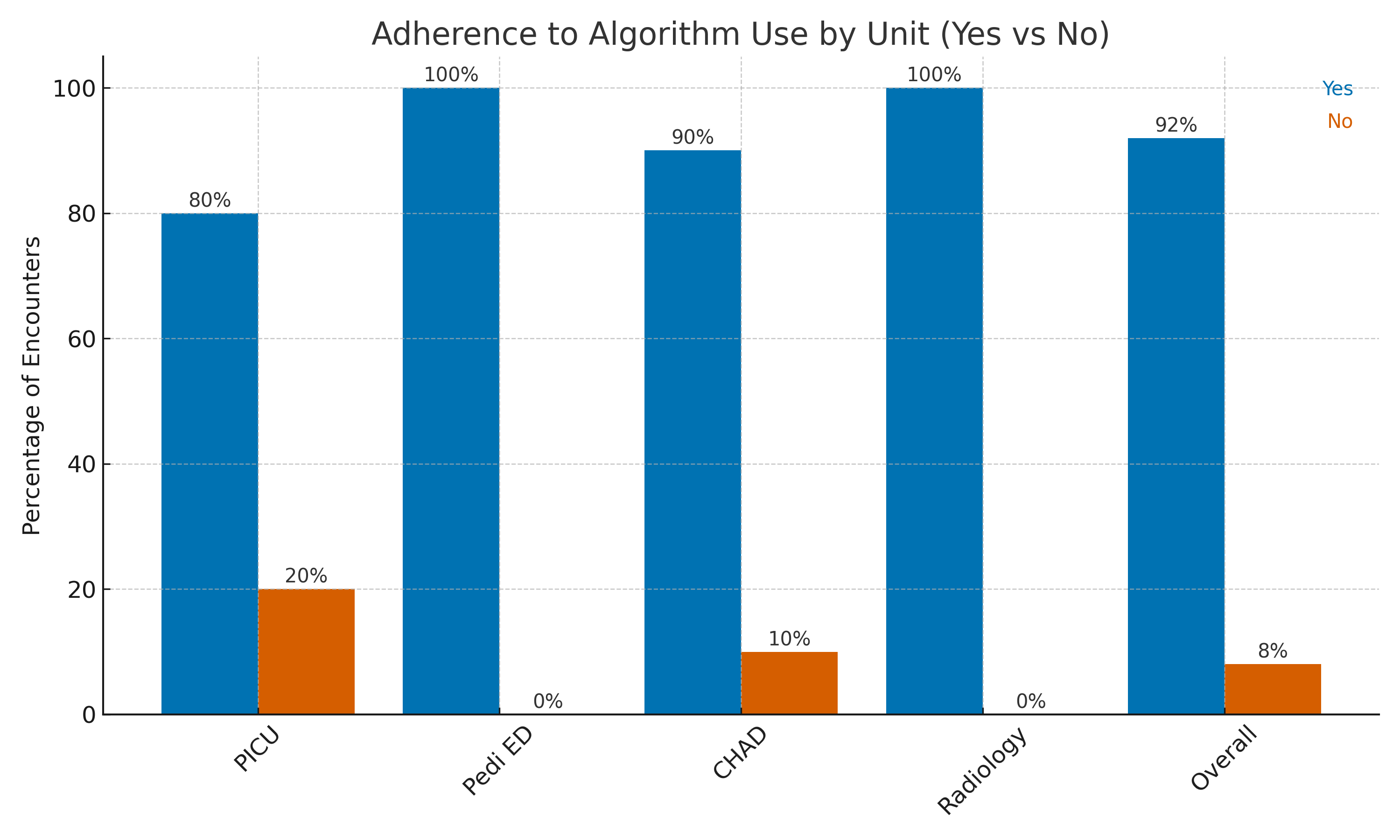
Results: Baseline included 777 patients, 1,010 IVs, and 1,266 attempts (mean 1.63 sticks/patient). Children ≤2 years required more attempts than ages 3–21 years (2.1 vs 1.4, p< 0.00001). Six percent required ≥4 attempts, and 5% of encounters needed cross-unit support, usually PICU staff. Thirty nurses and eight residents completed ultrasound training.In the 2025 pilot, 758 pre-intervention and 134 post-intervention patients were analyzed. Mean sticks/patient changed as follows (pre→post): PICU 1.85→1.75; Radiology 1.04→1.18; Pediatric ED 1.12→1.23; CHAD 1.45→1.60; overall 1.29→1.38 (Figure 1). Run charts showed fewer extreme outliers but persistent unit-level variation. Early trends likely reflect that the DIVA score was not yet embedded in CIS, and the guideline, escalation pathway, and comfort-measure workflow were new processes. Hospital staffing transitions also limited reinforcement and reliability.Despite these challenges, DIVA documentation and escalation adherence improved during the pilot with an overall 92% adherence rate (figure 2). Ultrasound use also increased. As DIVA scoring becomes integrated into CIS and training stabilizes, clearer reductions in mean attempts are anticipated.
Conclusions: Baseline evaluation demonstrated significant PIV burden and system gaps across pediatric units. Early implementation of a DIVA-based guideline was feasible but showed variable impact due to incomplete CIS integration and workflow adoption. A second cycle of data collection following full CIS integration, sustained education, and expansion of ultrasound capacity is expected to yield stronger and more consistent improvement in PIV outcomes.
.png)