Background: Readmissions within 30 days of discharge is used as a quality metric for the care of hospitalized patients. However, its prognostic value for patient outcomes has not been examined. We hypothesized that patients who get readmitted within 30 days of their index admission discharge may have higher short and long-term mortality.
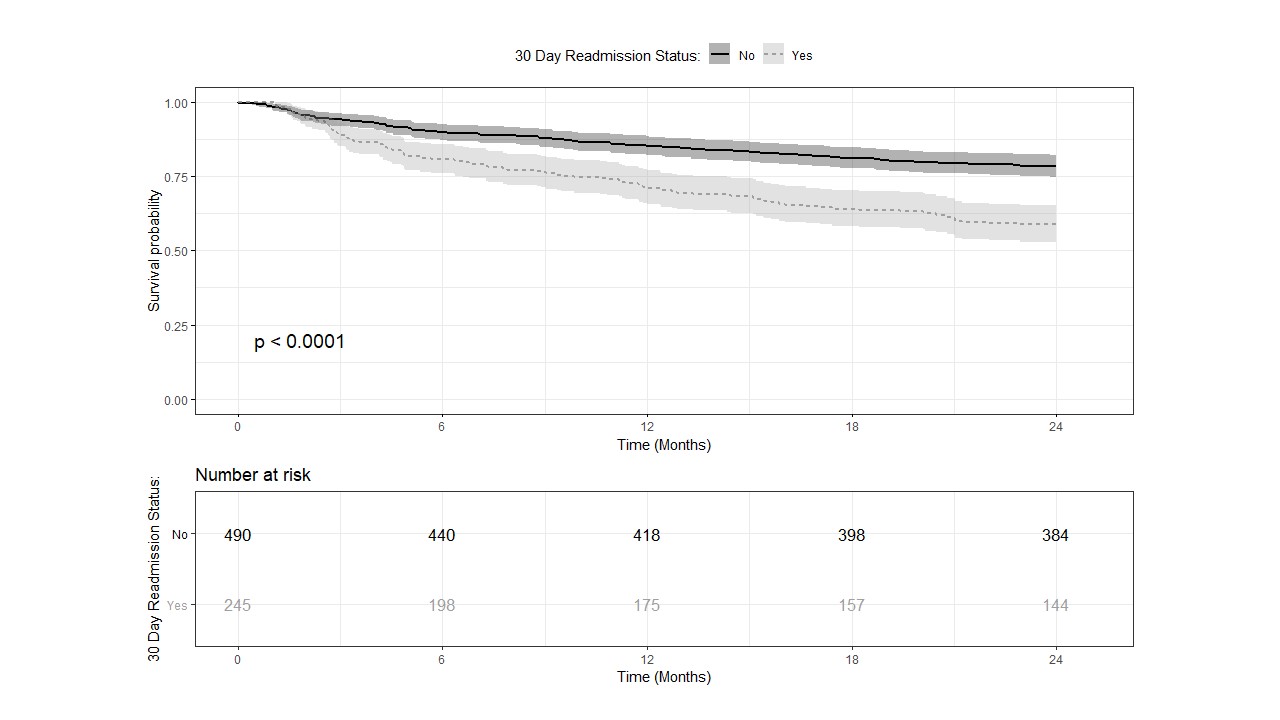
Methods: Using administrative data at a Veterans Affairs hospital, we retrospectively analyzed 2,353 unique patients admitted to the hospital on the inpatient medicine service over a period of one year. Patients with readmissions within 30-days of discharge were identified. The patients were matched for Diagnostic Group (DRG) and Severity Index (SI) using nearest propensity scores in a 2:1 ratio of non-readmission to readmission within 30-days post discharge. The final matched sample size was reduced to 735 patients with 490 in the non-readmitted (NRA) and 245 in the readmitted (RA) patients. Patients were followed at 6, 12, 18 and 24 months for all-cause mortality. A Kaplan-Meier curve was plotted against the two groups and a stratified log-rank test was performed to evaluate the overall difference between the two curves (Fig.1)
Results: The mean age of NRA patients was 67.6 ± 12.2 years and that of RA patients was 68.4 ± 13.4 years (p=0.42). Majority of patients in both groups were males with matched race and ethnicity. The mean length of stay between NRA and RA was not statistically significant (4.4 ± 4.6 days vs 4.5 ± 4.3 days respectively; p=0.59). The top three DRG for the matched sample for the two groups were similar including cardiovascular, gastrointestinal, and infection. The survival probabilities were consistently greater across all the time points 6, 12, 18 and 24 months for the patients who were not readmitted within 30-days of the index admission. The stratified Cox proportional hazard model yielded a hazard ratio of 2.06 for 30-day readmissions (95% CI of 1.55, 2.74; p=<0.001).
Conclusions: Readmission within 30-days after discharge is an independent risk factor for all-cause mortality which persists for at least 2 years independent of DRG or SI. Resource allocation to this high-risk patient group may help to decrease mortality and improve health outcomes.