
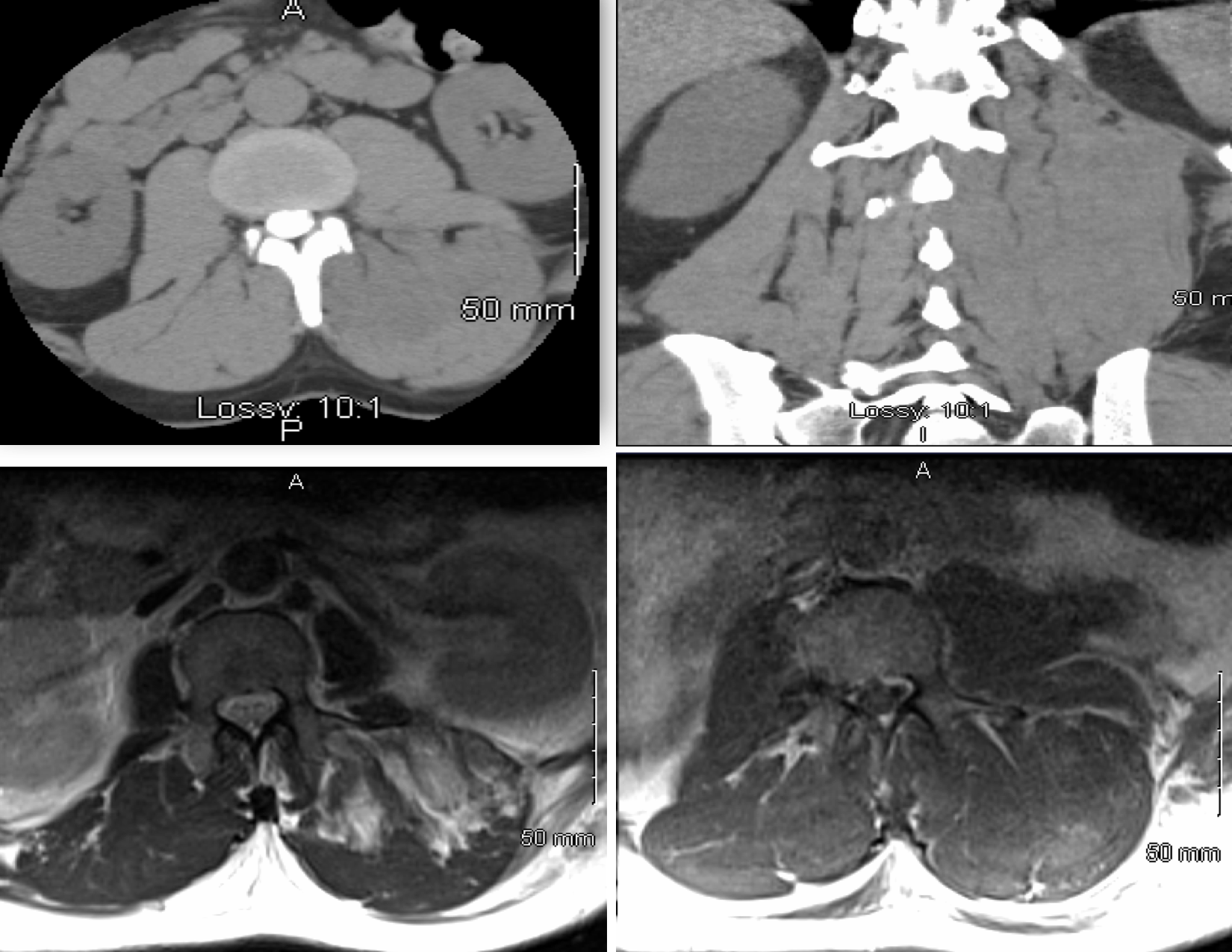
Case Presentation: A 43-year-old black man presented with acute onset back pain and lower extremity weakness for 6 hours. He admitted to intranasal heroin use 8 hours before. He awoke to severe sharp, continuous back pain, worse on the left lateral aspect of the back without any radiation and inability to stand or bear weight due to severe weakness and paresthesias.He denied urinary and fecal incontinence, perineal hypoesthesia/anesthesia, trauma, fever, chills or oliguria. On physical exam, vital signs are within normal limits. On musculoskeletal exam, found to have left lumbar paraspinal firmness and tenderness to palpation. On Neurological exam , strength was 0/5 left lower extremity, 0/5 right hip flexors and extensors, 2-3/5 right flexors and extensors of knee and ankle. On sensory exam: decreased light touch sensation in the lower extremities, more prominent over the left peroneal distribution. No sacral hypoesthesia/anesthesia. Reflexes: absent in lower extremities. Rectal tone: preserved. Laboratory exam is updated in the table listed below. Paraspinal abscess was suspected, patient was admitted to ICU and treatment with vancomycin and piperacillin-tazobactam plus intravenous steroids was initiated. Hemodialysis was initiated for severe rhabdomyolysis with acute anuric renal failure. Magnetic resonance imaging (MRI) and CT myelogram of the spine with contrast showed edema of left paraspinal muscle involving erector spinae and left gluteus muscle without evidence of nerve or cord compression, epidural abscess or spinal stenosis. Transferred out of ICU, weakness unchanged, myositis vs compartment syndrome suspected. Tissue pressures in the left paraspinal and gluteal region were measured as 45 mm Hg and 75 mm Hg respectively confirming compartment syndrome. He was transferred to a tertiary care facility where urgent fasciotomy was performed. Intraoperative findings included ischemic and necrotic left erector spinae muscle which required debridement, as well as viable left gluteus muscle without ischemia.
Discussion: Acute compartment syndrome is most commonly seen in the lower extremities, it is rarely seen in the paraspinal and gluteal compartments and can be a diagnostic challenge. Most cases are attributed to direct trauma. Atraumatic causes include weight lifting, downhill skiing, surfing and non-spinal surgery (aortic bypass, aneurysm repair, gastric bypass); rarely substance abuse via cytotoxic effects. Presentation varies but common symptoms include acute onset back pain, neurological symptoms, rhabdomyolysis and renal failure. Diagnostic modalities include MRI and computed tomography myelogram but MRI is more sensitive. Direct measurement of compartment pressure remains the gold standard. Paraspinal compartment pressures of 70-80 mm Hg and gluteal pressures less than 30 mmHg are considered normal by some sources.
Fasciotomy is the treatment of choice as untreated compartment syndrome has serious complications including irreversible neurologic impairment and even death.
Conclusions: Early diagnosis and treatment of paraspinal and gluteal compartment syndrome is of utmost importance. A high index of suspicion is necessary to ensure early diagnosis. Urgent fasciotomy with debridement is critical in preventing devastating neurologic sequelae and death.
.png)