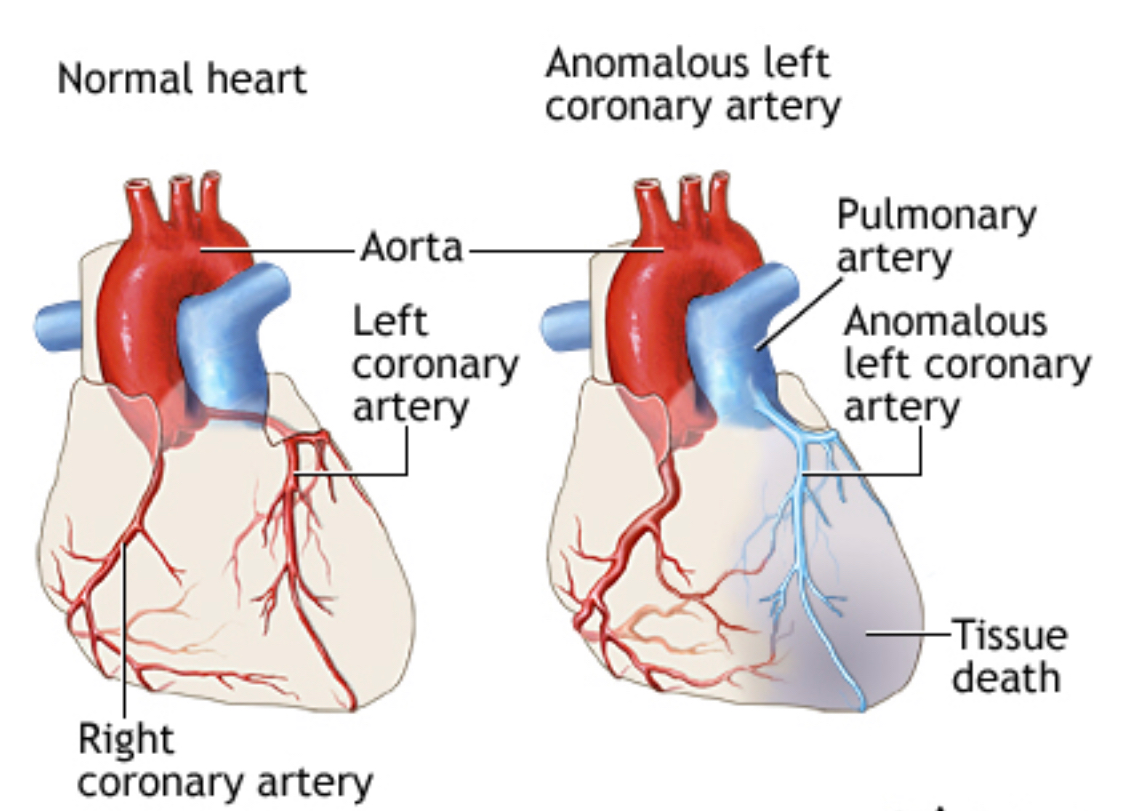
Case Presentation: Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) is a rare congenital anomaly usually presenting in infants with high mortality. This is a one of the rare cases of ALCAPA diagnosed at 40 years of age which presented with a series of complications after repair of the anomaly.Case: A 60-year-old female presented complaining of chest discomfort. 17 years ago she had a cardiac catheterization after a positive stress test for exertional dyspnea and chest pain. Cardiac catheterization revealed an anomalous connection between left anterior descending coronary artery (LAD) and pulmonary artery (PA). This was surgically corrected. At 6 month follow up, a transthoracic echocardiogram showed pulmonic valve gradient of ~50 mmHg. Follow up cardiac catheterization in 2002 confirmed presence of supravalvular pulmonic stenosis and 25-40% left anterior descending artery (LAD) stenosis. In 2004, she was admitted for worsening dyspnea and was found to have worsening pulmonic stenosis. In 2011, she had a positive nuclear stress test for chest pain. Subsequent cardiac catheterization revealed 90% stenosis in the first diagonal branch of LAD. A bare metal stent was placed. In 2014 she presented with worsening chest pain; cardiac catheterization showed diffuse 60% in-stent stenosis in the D1 branch of LAD, she was managed medically. In 2017 she presented with recurrent chest pain. A stress test was done but was aborted due to a wide complex tachycardia and subsequent cardiac catheterization showed severe supravalvular pulmonic stenosis, worsening right heart pressures and tricuspid regurgitation. She underwent pulmonic valve replacement in September of 2017. She recovered from the surgery but on March of 2018 she developed sudden cardiac arrest and died.
Discussion: ALCAPA, is a rare congenital anomaly, with an incidence of 1 in 300,000 live births accounting for 0.25 to 0.5 % of all congenital heart defects. Left untreated, it carries 90% mortality within one year of age. About 10-15% survive into adulthood due to extensive collateral circulation. Patients who survive into adulthood are at increased risk of myocardial infarction, left ventricular dysfunction, mitral insufficiency, malignant dysrhythmias or silent myocardial ischemia which can lead to sudden cardiac death (80-90%). CT or MR angiography can be useful in the diagnosis. Surgical correction by translocation is the standard of care with the goal of restoring two-coronary-artery circulation. ALCAPA patients are high risk of CAD, mitral valve regurgitation, heart failure and risk of sudden cardiac death. This case is unique as she developed progressive supravalvular pulmonic stenosis with progressive right heart failure needing pulmonic valve placement.
Conclusions: Coronary anomalies should also be considered in the differential diagnosis of adult patients presenting with ischemic heart disease symptoms. It is also important to promptly refer for surgical intervention when appropriate. In ALCAPA close follow up is critical to monitor for complications such as supravalvular pulmonic stenosis and coronary artery disease which places the patient at an increased risk of fatal arrhythmias.