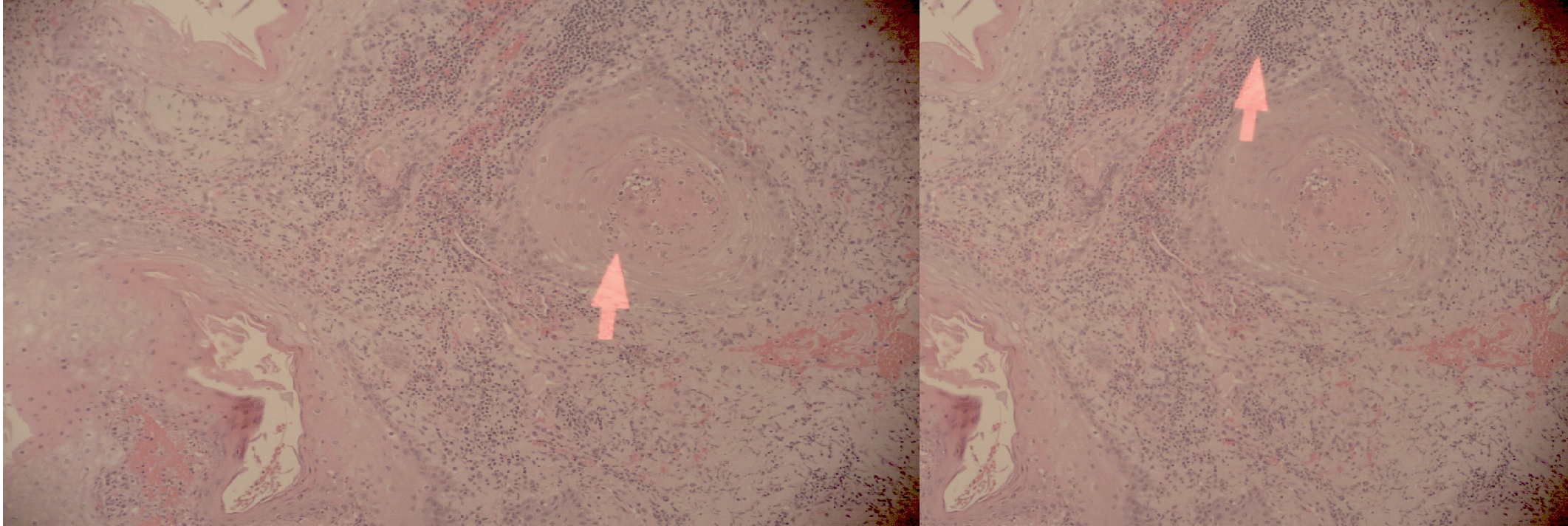
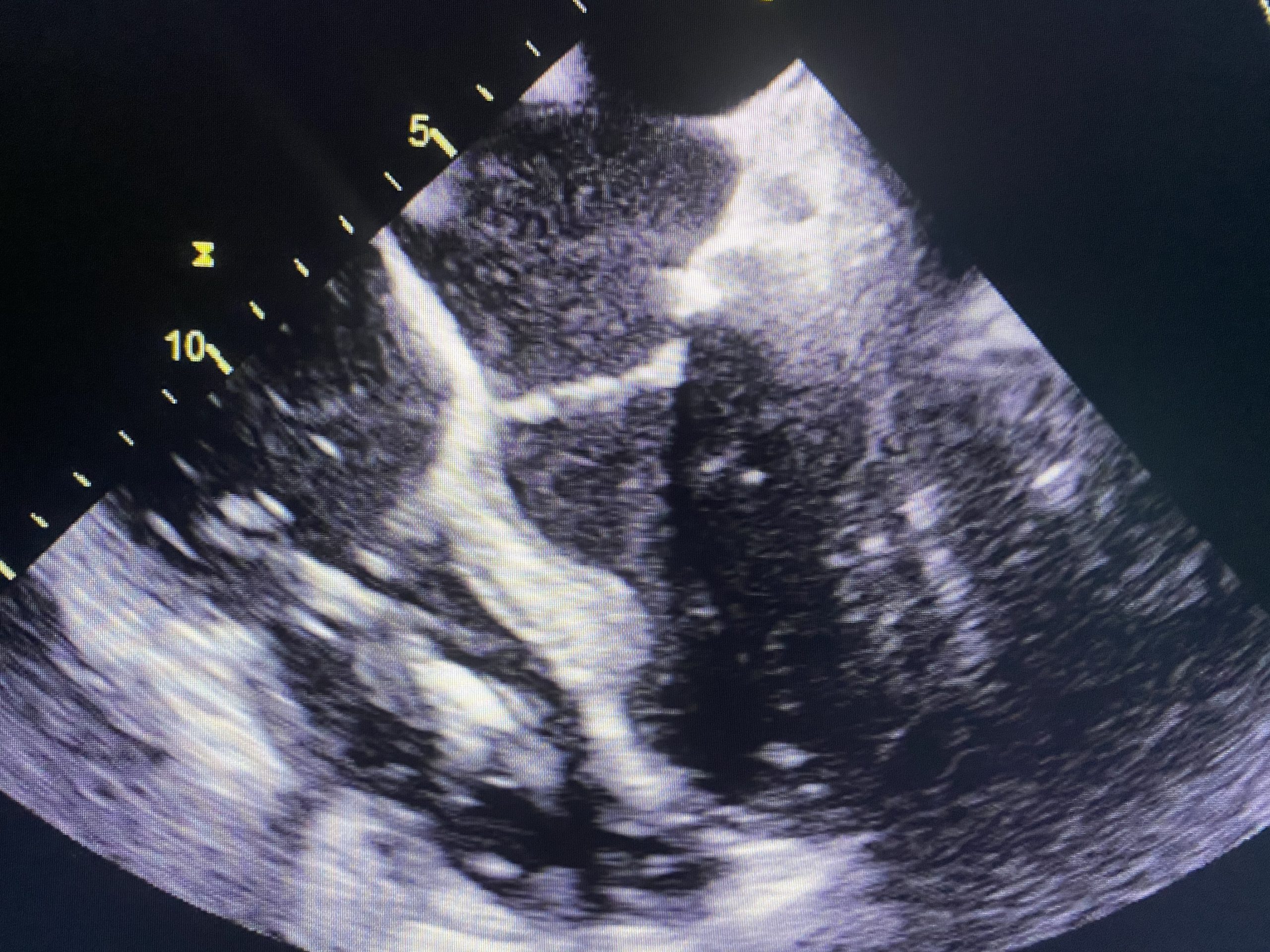
Case Presentation: This is the case of a 77-year-old male who was treated for endocarditis that seeded from a chronic upper extremity wound. The patient had a history of chronic atrial fibrillation and was status post placement of an AICD pacemaker. He initially presented to a community hospital with altered mental status and was found to be bacteremic with Methicillin-resistant Staphylococcus Aureus (MRSA) isolated on culture. He remained persistently bacteremic despite appropriate antibiotic therapy. A transesophageal echocardiogram demonstrated vegetations on his tricuspid valve and pacemaker wires. He was then transferred to a cardiology and vascular surgery-centered inpatient facility where our team assumed care. On admission, the patient was noted to have a 3 cm by 2 cm non-healing wound on his right upper extremity with purulent drainage and eschar that also grew MRSA on culture. He underwent surgical extraction of his AICD device when intravenous vancomycin therapy yielded sterile blood cultures. The culture of the AICD also yielded MRSA. At the same time, the eschar on his upper extremity was debrided and biopsies were sent to pathology. The pathology report showed cutaneous squamous cell carcinoma. The patient received a replacement biventricular ICD when his blood cultures were sterile. He was referred to outpatient hematology/oncology for further management and was discharged on six weeks of vancomycin.
Discussion: A Marjolin ulcer is a chronic, non-healing wound that undergoes a malignant transformation. Classically, the term describes squamous cell carcinoma transformation of chronic burns scars, however, the definition now includes any malignant transformation of a chronic wound. Squamous cell carcinoma is the most common malignancy reported, however basal cell carcinomas have also been noted. The exact pathophysiology is unclear, but the degeneration is thought to be due to persistent inflammation causing the breakdown of healthy tissue and reduction of Langerhans cell activity. Squamous cell carcinoma development itself is linked to mutations in the RAS/RAF molecular pathway. The ulcers typically feature irregular borders and exophytic spread. Pathology of squamous cell carcinoma shows classic nests of keratin pearls that invade into the epidermis and dermis. The cancers, in the setting of Marjolin ulcer, are often aggressive and quickly invade locally. Treatment involves debridement or amputation of the affected area if cancer has spread deeply. The wounds over time can become infected if a patient repeatedly excoriates the area, often due to colonization of the wound by opportunistic infections. Methicillin-resistant Staphylococcal species are uncommon in infected ulcers, however, they can lead to osteomyelitis or endocarditis if untreated, as in the case of our patient. Infected ulcers require appropriate antibiotic therapy and debridement of the wound. Prompt recognition and treatment are important for the reduction of overall morbidity and mortality in these cases.
Conclusions: The authors present this case to emphasize the importance for clinicians to be aware and intervene accordingly when a patient presents with a non-healing wound. The lesions can become malignant and are at risk of infection when the patient repeatedly excoriates the area, putting the patient at an increased risk of hematogenous spread, and complications like osteomyelitis and endocarditis.