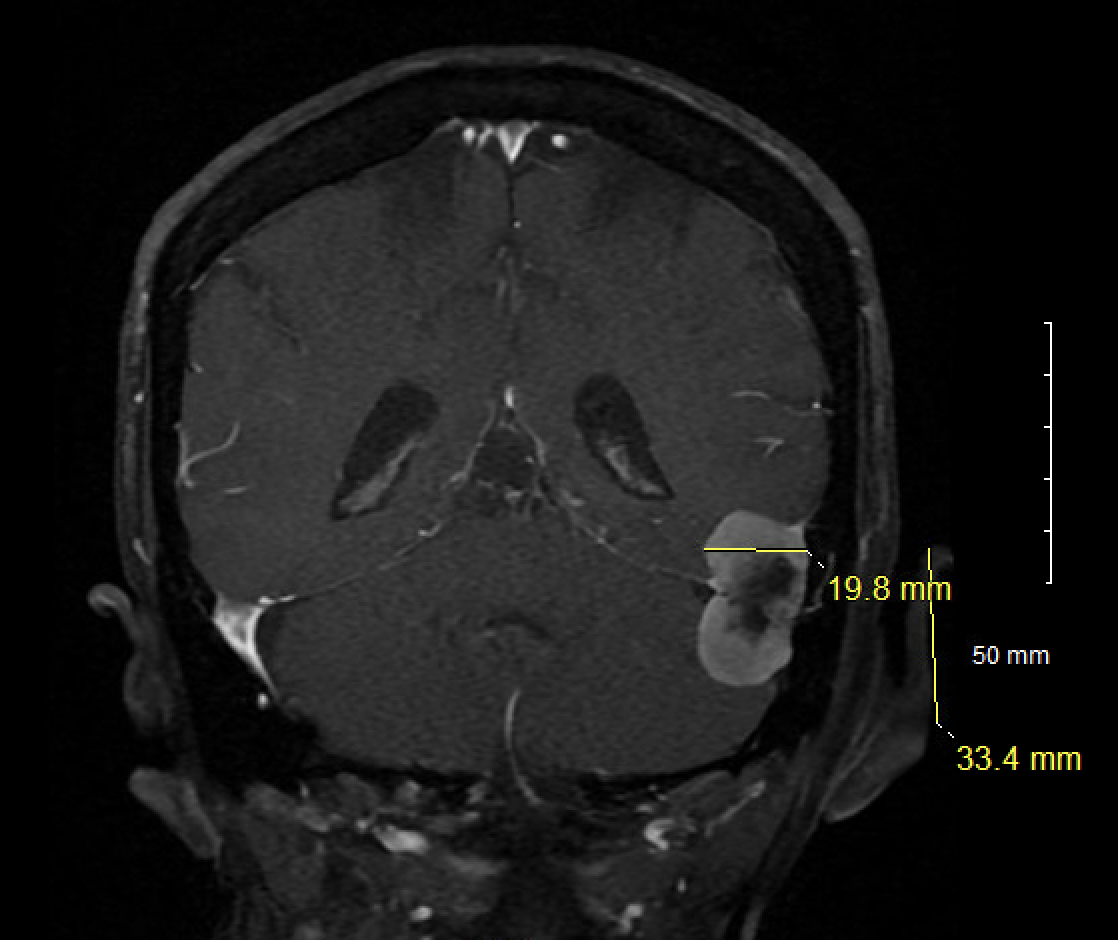
Case Presentation: A 75-year-old female with dementia, hypertension, hypothyroidism, and meningioma presented with altered mental status. The family reported declines in the patient’s memory, gait, and depth perception in addition to poor appetite, visual hallucinations, and vision changes. To them, her dementia has rapidly progressed and was far worse than baseline. On admission, the patient was diagnosed with UTI and treated with antibiotics with no improvement. Other lab-work, including vitamins D, B1, B12, B9, zinc, and copper were normal. Given visual disturbances, Ophthalmology was consulted and the patient was noted with left homonymous hemianopsia. They recommended neurology consult and stroke work-up. Head CT was negative for infarct, CT angiogram of head and neck showed no major vessel occlusion, and brain MRI showed a stable meningioma for which neurosurgery recommended against surgical intervention. EEG showed mild-to-moderate diffuse cerebral dysfunction consistent with encephalopathy. Geriatrics was consulted and delirium precautions were placed, Donepezil dosage was increased, and Sertraline and Quetiapine as needed were added for mood and agitation, respectively. The patient’s health-care proxy was activated given her poor insight and decision-making capacity. The patient’s mental status continued to decline and she was noted with new neurologic deficits: bilateral upper-extremity tremors, lip twitching, and oropharyngeal dysphagia. Repeat MRI and EEG remained unchanged. Lumbar puncture was performed for infectious, autoimmune and paraneoplastic evaluation. CSF meningitis panel, autoimmune and paraneoplastic antibody panels were negative. However, 10 days into admission, prion-specific biomarker studies revealed CSF 14-3-3 protein of 40,047 AU, total tau of 5,468 pg/mL, and a positive RT-QuIC assay, consistent with prion disease. Given poor prognosis, the family elected to pursue comfort measures. The patient was made DNR/DNI, and discharged to hospice.
Discussion: Rapidly progressive dementia (RPD) in the elderly remains an ongoing diagnostic dilemma given the list of differentials, including metabolic derangements, infections, medications, structural abnormalities, autoimmune disorders, paraneoplastic pathology, and, in rare instances, prion disorders. Sporadic Creutzfeldt–Jakob disease (sCJD), the most common prion disorder, involves a rapid cognitive decline and is associated with neurologic deficits such as myoclonus, personality changes, visual disturbances, gait dysfunction, or dysphagia. In the past, MRI and EEG were used for diagnosis, but recent use of CSF biomarkers including CSF 14-3-3 protein, total-tau, and the RT-QuIC assay have improved the pre-mortem diagnosis of prion’s disease with specificity exceeding 98% with the latter.
Conclusions: The case hones in on the diagnostic challenges in elderly patients with multiple co-morbidities that present with worsening dementia. The patient’s history of dementia, known meningioma, use of antipsychotics and serotonergic medications suggests multifactorial etiologies and delays the diagnosis of prion’s. Ultimately, it was not the neuroimaging or EEG, but the combination of prion-specific biomarker studies with a positive RT-QuIC assay that lead to a definitive diagnosis. Although the prognosis remains poor, this case emphasizes broadening one’s differential for RPD while also highlighting the use of prion assays to diagnose the condition earlier to transition to comfort-focused care.