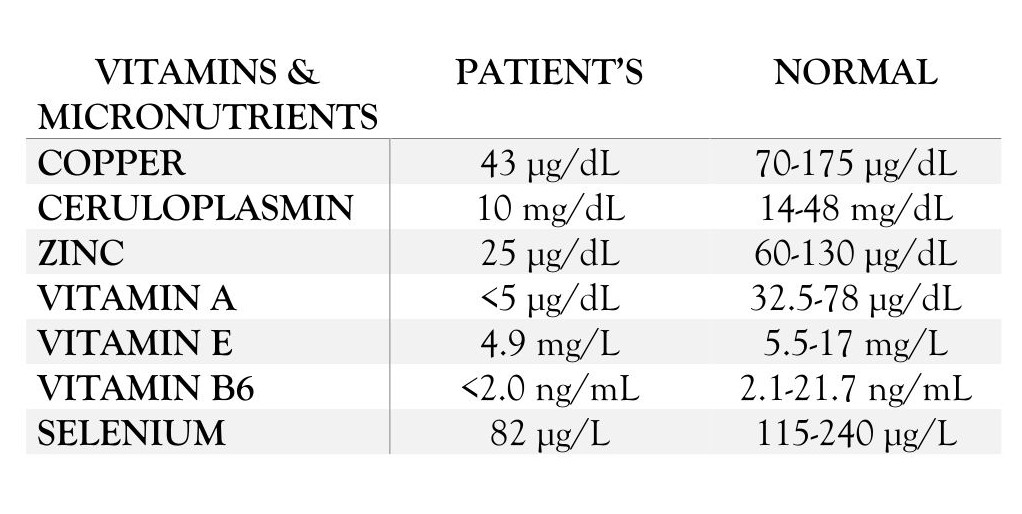
Case Presentation: A woman in her mid-30s with a past medical history of Roux-en-Y gastric bypass and hypothyroidism, presented with six months of progressive bilateral leg numbness and weakness, worsening confusion, abdominal pain, constipation, and intermittent rectal bleeding. She was febrile, tachycardic, and hypotensive with mild leukocytosis. CT of the abdomen showed stercoral colitis, and broad-spectrum antibiotics were started. Her mental status and hemodynamics declined, prompting ICU transfer for concern of septic versus hemorrhagic shock. MRI, EEG, and lumbar puncture were unrevealing, and infectious, autoimmune, and paraneoplastic studies were negative. Thyroid studies and heavy-metal screening were normal.Labs showed macrocytic anemia with hemoglobin 7.7 g/dL (11.6-15.4) and MCV 105 fL (80-99). She had marked micronutrient deficiencies: copper 43 µg/dL (70-175), ceruloplasmin 10 mg/dL (14-48), zinc 25 µg/dL (60-130), vitamin A < 5 µg/dL (32.5-78), vitamin E 4.9 mg/L (5.5-17), vitamin B6 < 2.0 ng/mL (2.1-21.7), and selenium 82 µg/L (115-240). Vitamin B12 and thiamine were elevated. Wilson’s disease testing was negative. A 24-hour urine copper of 132 µg/24 h (9-71) suggested malabsorption. Ammonia levels intermittently rose to 104 µmol/L (11-60), and she received lactulose and rifaximin. High-dose steroids were initially administered for possible autoimmune encephalitis but discontinued after deficiency-mediated encephalopathy was suspected. Fecal elastase levels were low, and pancreatic enzyme therapy was initiated. She received vitamin and trace-element repletion with neurological improvement.Her course was further complicated by rectal ulcer bleeding, coagulopathy, and anemia requiring transfusions and endoscopic clipping, aspiration pneumonia with ARDS requiring mechanical ventilation and tracheostomy, and prerenal acute kidney injury requiring CRRT. She was ultimately stabilized and discharged to rehabilitation.
Discussion: This case shows how severe micronutrient deficiency can cause encephalopathy and neuropathy years after gastric bypass. While B12 deficiency is well known, copper, zinc, and B6 deficiencies are often missed despite their potential to cause profound neurologic and hematologic problems. Copper deficiency may mimic demyelinating disorders with myeloneuropathy and anemia, while low zinc and B6 can further exacerbate neurological dysfunction. Her critical illness and overlapping symptoms initially masked the nutritional cause and led to a search for autoimmune and infectious explanations. Her recovery after targeted repletion highlights the need to consider micronutrient deficiency in post-bariatric patients with unexplained neurologic changes or cytopenias.
Conclusions: Micronutrient deficiency is an underrecognized but reversible cause of encephalopathy and neuropathy in patients with a history of gastric bypass. Hospitalists should remain alert to copper, zinc, and B6 deficiencies, as timely recognition and replacement can prevent permanent neurologic injury.