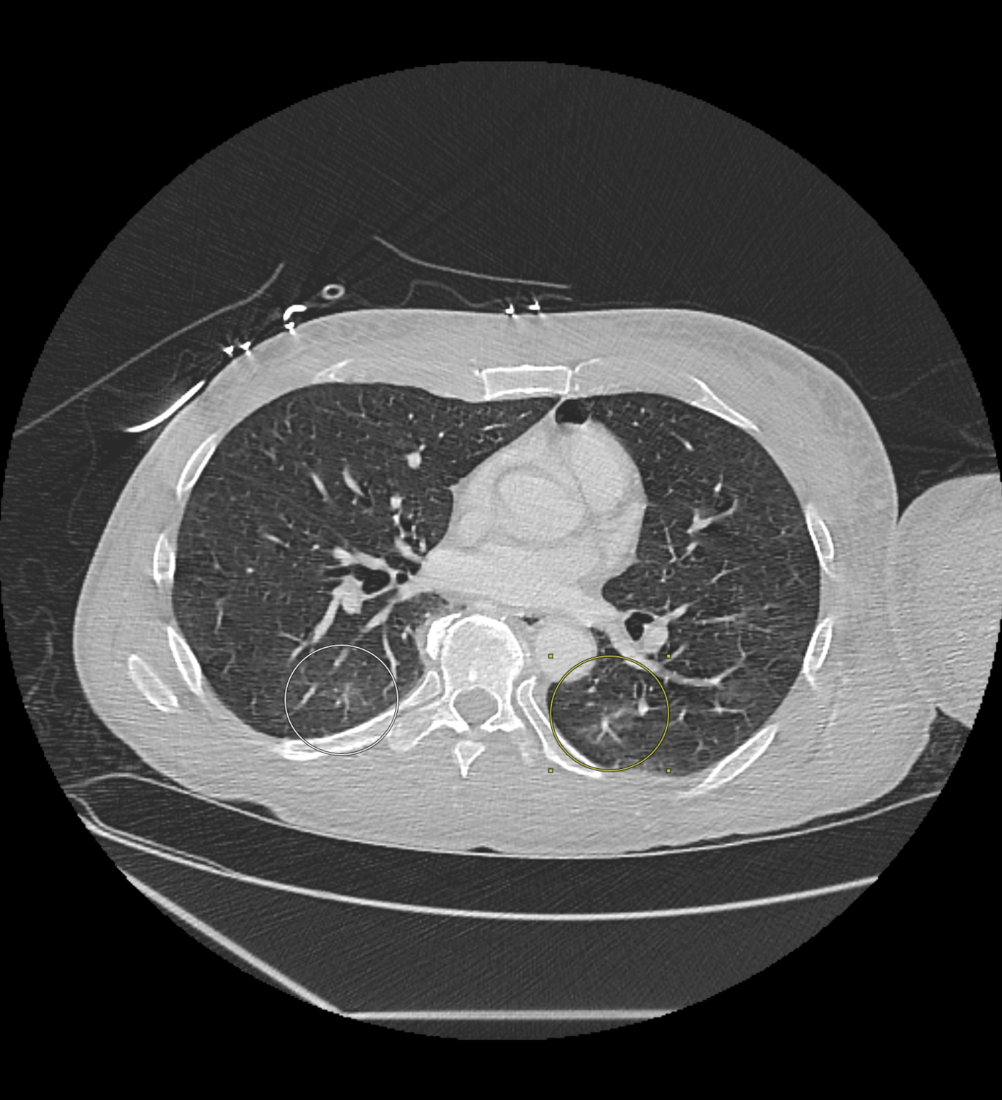
Case Presentation: A 59-year-old unhoused man presented with three days of progressive left arm pain and swelling after a spider bite sustained while sleeping outdoors. He reported two puncture marks followed by severe 9/10 pain and rapidly worsening edema. His history included type II diabetes, hepatitis C cirrhosis, autoimmune skin disease, and polysubstance use disorder. Examination revealed a 1 cm ulcerative lesion on the volar wrist with purulent drainage, circumferential erythema, and coolness of the distal forearm. Radial pulse and capillary refill were intact. CT imaging demonstrated diffuse subcutaneous edema without organized abscess (Fig. 1). He was started on piperacillin–tazobactam and linezolid and underwent emergent fasciotomy, debridement, and carpal tunnel release. Intraoperatively, the tissue appeared woody and scarred without muscle necrosis. Wound cultures grew Clostridium perfringens, confirming clostridial necrotizing infection.Despite immediate intervention, his condition deteriorated rapidly. By postoperative day 2, he developed severe abdominal pain, metabolic acidosis, rhabdomyolysis, disseminated intravascular coagulation, and shock liver. Further CT revealed mesenteric ischemia, and exploratory laparotomy showed diffuse bowel necrosis requiring multiple resections, cholecystectomy, and ileostomy. Subsequent CT chest demonstrated bilateral ground-glass opacities consistent with acute lung injury secondary to systemic inflammation (Fig. 2). His course was further complicated by oligoanuric acute kidney injury requiring dialysis. At follow-up, he remained dialysis-dependent with limited renal recovery and a guarded prognosis due to extensive bowel loss, persistent renal failure, and unfavorable social barriers.
Discussion: Severe systemic illness from spider envenomation is exceedingly uncommon, as most cases are self-limiting. This case demonstrates how toxin-mediated tissue injury and secondary infection can synergize to cause catastrophic outcomes, particularly in medically and socially vulnerable populations with delayed access to care.Prior reports of spider envenomation have described transient myocarditis or localized necrosis [1, 2], but none with combined intestinal ischemia, lung injury, and renal failure. To our knowledge, this is the first reported case of spider envenomation complicated by imaging-confirmed anasarca and acute lung injury, with prior reports of arthropod-induced acute respiratory distress syndrome limited to scorpion and tick envenomation [3, 4]. It is also the first case linking spider bite to mesenteric ischemia, previously only described after massive wasp or snake envenomation [5, 6]. The patient’s medical fragility, chronic infections, and limited access to early intervention underscore how social vulnerability can transform a minor exposure into a life-threatening illness.
Conclusions: Spider bites rarely lead to necrotizing infections or multiorgan failure, but outcomes may be catastrophic in patients with medical or social risk factors. Clinicians should maintain high suspicion for necrotizing infection in rapidly progressive soft-tissue lesions, particularly in unhoused or immunocompromised individuals. Early recognition, timely surgery, and integrated care addressing social factors are key to preventing catastrophic outcomes—and to reminding clinicians that even minor wounds in vulnerable patients can hide major pathology.