
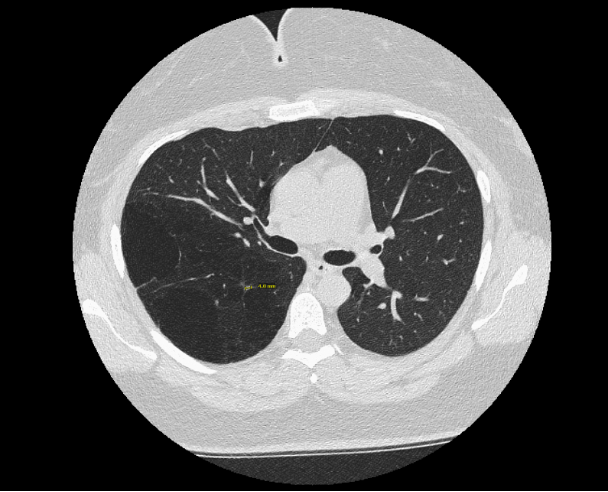
Case Presentation: A 39-year-old woman with obesity, PTSD, anxiety presented to the ED following a high-speed motor vehicle accident. Comprehensive trauma CT imaging showed no acute traumatic injury; however, CT chest revealed multiple large bullae confined to the right lung, predominantly within the lower lobe, initially raising concern for placental transmogrification (Fig. 1). She was a lifelong never-smoker with a 2-year history of progressive exertional dyspnea previously attributed to mild sleep apnea by her PCP. Pulmonology evaluation demonstrated mild airflow obstruction (FEV1 73%, FEV1/FVC 0.68) with severe air trapping (RV 207%, TLC 113%) and preserved diffusion capacity (Fig. 2). Given the lesion’s unilateral nature, she underwent a right lower lobectomy with a right upper lobe wedge resection. Histopathology revealed multilocular respiratory-epithelial–lined cyst with ciliated columnar epithelium, variable smooth muscle, and focal fibrosis, favoring congenital pulmonary airway malformation (CPAM) type 1. Follow-up imaging showed minimal residual emphysema, and she remained clinically stable on budesonide–formoterol, nasal steroids, weight-loss therapy, and pulmonary rehabilitation.
Discussion: CPAM is a congenital cystic lung malformation typically diagnosed in utero or early childhood; adult presentation is rare and often occurs incidentally or in the setting of complications such as infection or pneumothorax [1]. Given its characteristics, CPAM may closely mimic emphysematous disease radiographically, contributing to diagnostic uncertainty [2]. In this case, the lesion was identified only because of trauma imaging, despite several years of progressive dyspnea. The initial concern for placental transmogrification underscores how radiologic findings alone can be misleading, particularly for rare cystic lung disorders. Surgical pathology was ultimately required to clarify the congenital nature of the lesion and exclude malignancy. Because adult-diagnosed CPAM is uncommon, unfamiliarity with its radiographic patterns may heighten patient anxiety and delay appropriate evaluation. Additionally, her relatively subtle symptoms likely contributed to the delayed recognition of this underlying congenital abnormality.
Conclusions: This case highlights the challenges posed by incidental findings, the central role of hospitalists in navigating diagnostic uncertainty, and the importance of a thorough workup of dyspnea. Incidental discoveries, such as this patient’s unilateral bullous imaging, often lack clear clinical pathways and can mimic other conditions. Because imaging alone can be misleading, internists play a key role in determining which findings warrant further evaluation, coordinating multi-disciplinary specialty input, and guiding patients in managing the anxiety that accompanies unclear results. This case also underscores the diagnostic limitations of imaging alone and the value of multidisciplinary consults in establishing an accurate diagnosis and guiding management.
.png)