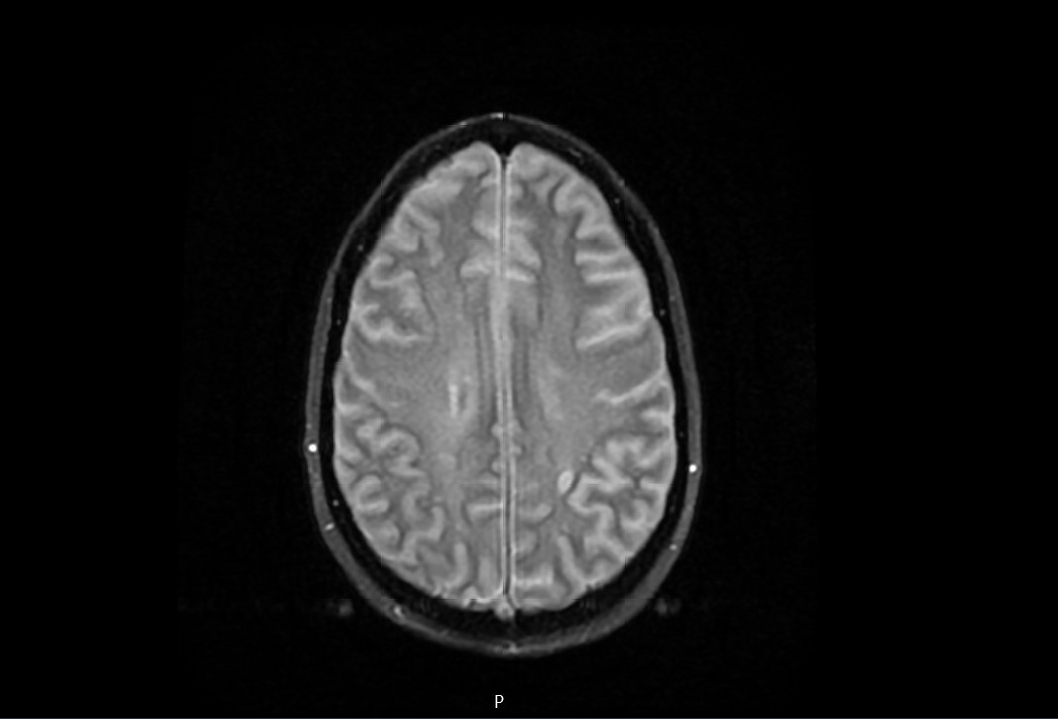
Case Presentation: 46-year-old female patient with a past medical history of ESRD on hemodialysis, DVT on chronic anticoagulation with apixaban, chronic HFrEF and history of injectable drug use (fentanyl) who presented with a chief complaints of progressive headache followed by rapidly progressive confusion requiring intubation for airway protection. Diagnostic lumbar puncture was considered however deferred given apixaban coagulopathy and thrombocytopenia. Empirical broad-spectrum antibiotic therapy along with acyclovir was initiated for suspicion of meningitis/encephalitis. CT head within 12 hours of presentation suggested evolving cerebral edema and CT angiogram of the head revealed diminished anterior intracranial circulation. Patient was treated with hypertonic saline. MRI of the brain revealed diffuse global cerebral and cerebellar diffusion restriction without diffuse enhancement (suggesting against an infectious etiology) likely consistent with opiate drug abuse. EEG ruled out nonconvulsive status epilepticus. Clinical course and presentation was highly suspicious for fentanyl induced leukoencephalopathy which can cause diffuse cerebral edema. Hospital course was complicated by hemodynamic instability requiring multiple vasopressor support and despite aggressive medical therapy, the patient continued to deteriorate clinically. Follow-up CT revealed catastrophic cerebral edema with complete effacement of all ventricles and sulci with evidence of transtentorial herniation. NM brain scan SPECT demonstrated an absence of cerebral perfusion. Serial brain death examinations demonstrated absence of all brainstem reflexes and cortical function without any confounding conditions and brain death was eventually declared.
Discussion: Opiate induced toxic leukoencephalopathy (TLE) is a rare and life-threatening complication of fentanyl overdose which is frequently under-recognized. Pathophysiology involves damage of brain white matter with myelin sheath injury. Clinical manifestations range from mild confusion to stupor, coma, and death. Prognosis depends upon the degree of damage. Differentials including hypoxic, ischemic, vascular, metabolic and infectious causes should be ruled out by comprehensive clinical evaluation, imaging, and lab testing (LP, EEG). Management is usually supportive, focusing on controlling intracranial pressure to avoid neurological complications with limited role of hyperosmolar therapies and corticosteroids. Severe cases may require intubation for airway protection and emergency neurosurgical intervention.
Conclusions: The opioid crisis and fentanyl overdose deaths is a significant public health concern. Given the rise in illicit fentanyl use, clinicians should have a higher index of suspicion for TLE in cases of unexplained acute encephalopathy presenting with classical history and neuroimaging findings. Furthermore efforts should be made for inclusion of fentanyl in routine urine drug screens for early diagnosis which can potentially improve outcomes.