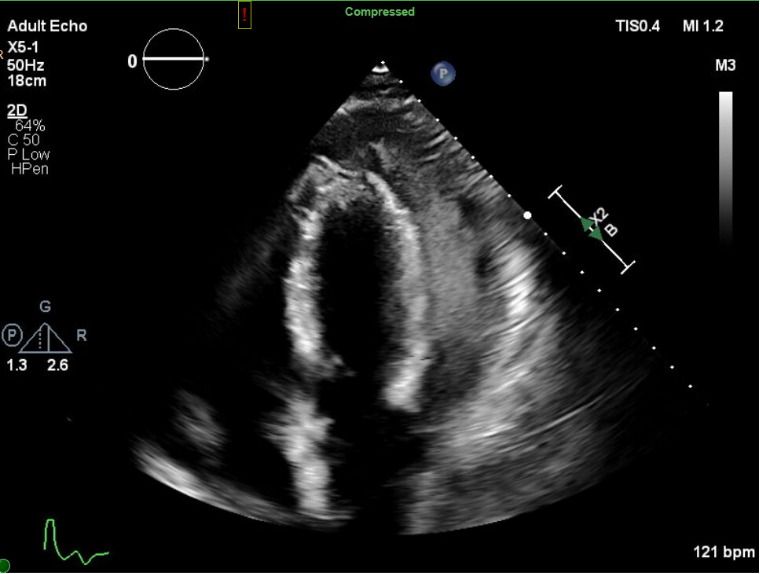
Case Presentation: A 33-year-old previously healthy man presented with fever, diffuse joint pain, muscle pain, and weakness after a recent gastrointestinal illness. Musculoskeletal exam revealed generalized muscle weakness and asymmetric synovitis involving large and small joints. Initial differential diagnosis included reactive arthritis given his recent diarrhea, though his presentation prompted concern for sepsis due to tachycardia, elevated lactate, and distant heart sounds. Blood cultures were drawn with two of two bottles positive for Haemophilus influenzae (H. influenzae). He was subsequently started on IV ceftriaxone. Shortly after IV fluid resuscitation, he developed dyspnea and pleuritic chest pain. EKG demonstrated diffuse ST-segment elevations consistent with pericarditis. Point-of-care ultrasound showed a pericardial effusion, prompting a formal echocardiogram. Findings included a large, loculated pericardial effusion with tamponade physiology (Figure 1). Cardiology performed an emergent pericardiocentesis with the removal of 600 milliliters of purulent fluid with greater than 50,000 nucleated cells/hpf (Figure 2). His pericardial fluid culture was negative, but the purulent effusion was presumed to be secondary to H. influenzae. The effusion persisted on repeat echocardiogram, and he ultimately requiredpericardiectomy. The patient had an uncomplicated post-operative course and completed a 14-day course of ceftriaxone. After a short admission to inpatient rehabilitation, he was discharged home in good condition. Given his presentation with invasive H. influenzae, HIV screening was sent andreturned positive. His CD4 count was 256/mm3, with a viral load of 25,000 copies/mL. He was started on anti-retroviral therapy, and at follow-up three months later, his CD4 count had improved and his viral load was undetectable.
Discussion: Purulent pericarditis is a rare bacterial illness in the post-antibiotic era. In adults, Staphylococcus aureus, Streptococcus spp., Haemophilus, and Mycobacterium tuberculosis are among the most common causes. In developed countries, purulent pericarditis accounts for less than 1% of allpericarditis cases, though immunocompromised patients remain at higher risk for this condition. Notably, patients with AIDS have an increased incidence of purulent pericarditis, particularly with Mycobacterium avium-intracellulare infection. Bacterial pericarditis presents as a rapidly progressive illness, with fever present in nearly all cases. The classic signs and symptoms associated with acute pericarditis (chest pain, friction rub, and pulsus paradoxus) are only seen in about 50% of patients, so a high index of suspicion is essential for diagnosis. If left untreated, the mortality rate approaches 85%, and it is reduced to 40% with treatment. Immunocompromised patients, as in our case, are at risk of rapid progression to tamponade. Therefore, high clinical suspicion and early detection are critical for reducing morbidity and mortality.
Conclusions: Our patient’s initial presentation was atypical for invasive H. influenzae. Hospitalists should consider bacterial pericarditis in febrile patients with chest pain, particularly when accompanied by other features of pericarditis. Additionally, identification of unusual pathogens should prompt evaluation for underlying immunodeficiency, particularly HIV. Timely identification andmanagement of this rare, life-threatening condition are essential to optimize patient outcomes.