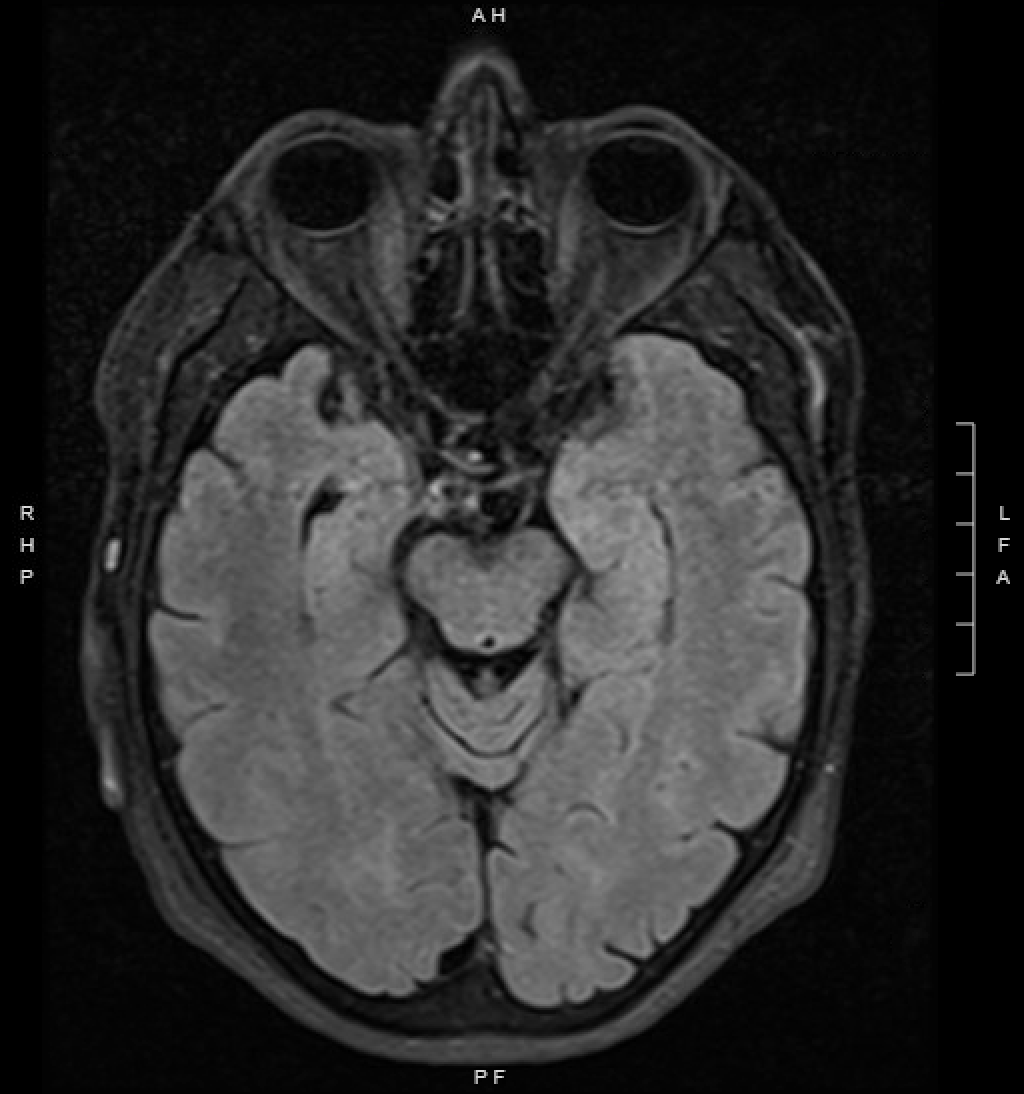
Case Presentation: A 59-year-old male with a past medical history of hypertension and cocaine use disorder presented to the emergency department for altered mental status (AMS) and weight loss. For two months he had been having progressively more frequent episodes of left facial grimacing with sudden flexion of the left arm. Additional symptoms included progressive difficulty with attention, short-term memory, behavior changes, and an unintentional 40-pound weight loss. He also reported smoking half a pack of cigarettes daily, consuming two drinks of alcohol per week, and using cocaine weekly. On arrival, his vitals were normal. His exam showed orientation to person and place but not time. He had bradyphrenia, a flat affect, difficulty with short-term memory, and was unable to perform serial sevens or spell “world” backwards. Initial laboratories revealed a normal glucose, normal blood gas studies, and moderate hyponatremia. A urine drug screen was positive for marijuana and cocaine. Brain MRI showed hyperintense areas in the bilateral temporal lobes. Next, a video-EEG was performed which demonstrated brief episodes of dystonic contraction of the face and ipsilateral arm suggestive of faciobrachial dystonic seizures (FBDS) without any electrographic correlates. These findings were concerning for LGI1 antibody encephalitis. To confirm the diagnosis a lumbar puncture was performed, and CSF studies were positive for LGI1-Igg antibodies. Initially, he was started on levetiracetam and IV methylprednisolone which was followed by a prolonged prednisone taper. After repeat EEG showed ongoing FBDS, plasmapheresis was trialed which also failed to improve his symptoms. He was then switched to lacosamide which resulted in both subjective and EEG evidence of decreased FBDS burden.
Discussion: LGI1 encephalitis is the second most common cause of autoimmune encephalitis following NMDAR-antibody encephalitis and is estimated to have a prevalence of .7 cases per 100,000 persons [1]. It presents with several unique features that help to distinguish it from other types of autoimmune encephalitis or AMS. The most characteristic clinical finding being that of FBDS which are pathognomonic for LGI1 encephalitis. These are a specific type of seizure which cause brief tonic contractions, typically of the arm and the ipsilateral face multiple times per day. These seizures present early in the disease course, prior to cognitive decline, and crescendo in severity 3-6 months after starting [2]. Other common symptoms include decline in short-term memory, behavioral disturbances, spatial disorientation, hyponatremia, and mesial temporal lobe hyperintensity on MRI [2]. LGI1 encephalitis typically responds well to immunotherapy with steroids being first line treatment. Plasma exchange, intravenous immunoglobulins, and rituximab are used as second line treatment options.
Conclusions: Altered mental status is one of the most common chief complaints admitted to the hospital. This case highlights the importance of keeping a broad differential in patient with AMS, even when they possess typical risk factors such as substance use, alcohol withdrawal, or electrolyte derangements. LGI1 encephalitis presents with typical prodromal symptoms, that if recognized quickly, can lead to early diagnosis and treatment.