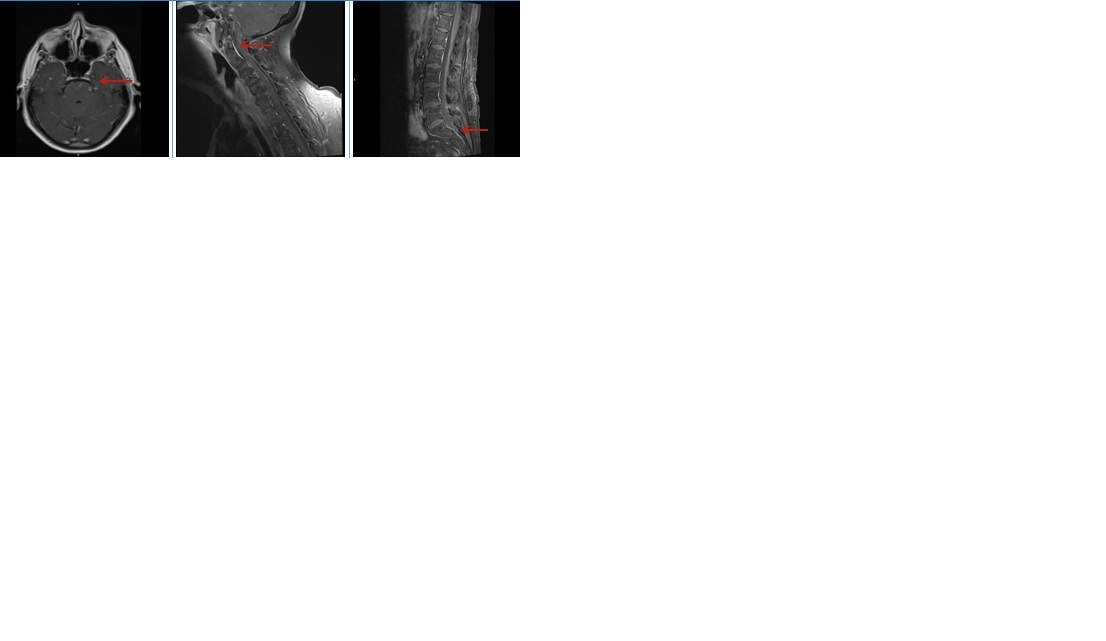
Case Presentation: A 72 y/o woman with hypertension and type 2 diabetes developed intermittent headaches, diplopia, ataxia, and confusion after participating in a Native American sweat lodge ritual in an enclosed tent. She lived on a farm, did frequent bush hogging; had not traveled outside of Texas in the last decade. Initial CT head was normal, but brain MRI revealed non-ischemic white matter changes and midbrain hyperintensities. EEG suggested partial seizures; levetiracetam was started but later discontinued after repeat normal study. As her cognition worsened, repeat MRI showed diffuse leptomeningeal enhancement. CSF analysis showed normal opening pressure, lymphocytic dominant pleocytosis, elevated protein, hypoglycorrhachia, ACE 2.8, and positive oligoclonal bands. Empiric ceftriaxone, vancomycin, and acyclovir were initiated. MRI brain and spine showed diffuse leptomeningeal enhancement, concerning for neurosarcoidosis. High-dose IV steroids were started for severe inflammation. CSF later tested positive for Blastomyces antibody. Treatment with liposomal amphotericin B was started with plans to transition to oral voriconazole or fluconazole for up to 1 year.
Discussion: CNS blastomycosis may present as meningitis, intracranial mass lesions, or spinal abscesses. Symptoms include headaches, altered mentation, visual changes, focal deficits, and seizures. CSF findings are pleocytosis, elevated protein, and low to normal glucose levels; cultures are often negative. MRI frequently demonstrates leptomeningeal enhancement. Isolated CNS disease is extremely rare, with only 7 cases reported since 1980, most in immunocompetent hosts. Our case is the first report of isolated CNS blastomycosis in Texas. The only other published case from Texas occurred in EL Paso in 2001, with pulmonary disease in an HIV patient, highlighting the rarity of our case. Standard therapy involves liposomal amphotericin B followed by prolonged azole therapy. Our diagnosis was delayed due to diagnostic confusion with neurosarcoidosis, as imaging and CSF findings overlapped significantly. Environmental exposures such as soil disruption during bush hogging and sweat lodge rituals may have served as possible sources. Our case highlights the shifting epidemiology of blastomycosis, suggesting clinicians in Texas and other historically non-endemic areas should maintain vigilance.
Conclusions: Blastomycosis, once thought limited to specific endemic regions, may be emerging in new geographic areas, including Texas. Though rare, isolated CNS disease can present in immunocompetent hosts, mimicking autoimmune or inflammatory conditions like neurosarcoidosis. Detailed environmental and social history is paramount in atypical CNS presentations. Ritual activities like sweat lodges represent unique exposure sources. Early recognition and antifungal treatment are critical for improved outcomes.