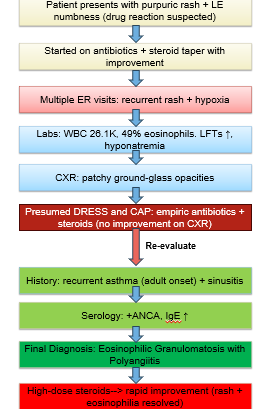
Case Presentation: A 53-year-old white male with the past medical history of psoriasis presented with purpuric rash on bilateral lower extremities for 4 days and numbness in the right foot. Within days of initiating Bactrim, he developed progressive rash involving upper extremities. He also started Tamsulosin for urinary retention. Rash was non-pruritic purpuric coalescing papules spreading to lower extremities. This was his 4th ER visit for this symptom and attributed each episode to new drug exposure and was empirically treated with antibiotics, oral or topical steroids and discharged. This time decision was made to admit patient for further work up. On presentation, he was hypoxic requiring 2L O2 via nasal canula. Initial work up showed WBC 26.15 comprising of 49% eosinophils, mildly elevated LFTs, and patchy ground-glass opacities on CXR bilaterally. Empiric antibiotics and steroids were initiated to cover for presumed community acquired pneumonia and DRESS. However, infectious work up was negative. Due to persistent rash without clinical improvement on prednisone alone, comprehensive evaluation revealed prior asthma diagnosis, multiple sinus infection visits, and clinical suspicion for EGPA. ANCA antibodies and IgE were positive. Outpatient dermatology biopsy demonstrated leukocytoclastic vasculitis with eosinophilic predominance, confirming EGPA. High-dose steroids were initiated with significant symptomatic improvement within 72 hours. He was discharged with rheumatology follow-up recommendations.
Discussion: This case exemplifies a rare but clinically significant diagnostic challenge where two distinct eosinophillic syndromes, EGPA and DRESS share overlapping features in presentation. Recent bacitracin and tamsulosin initiation masked the underlying EGPA pathology, resulting in anchoring bias towards DRESS. The average time to diagnose EGPA typically ranges from 2-9 years starting from the initial onset of asthma, which often presents in adulthood, to the vasculitis diagnosis. Diagnostic delay stems from the disease’s phasic progression (allergic, eosinophilic, and vasculitic phases). The full disease spectrum may not present initially, making early diagnosis challenging. Variability in presentation, including pulmonary, neurologic, cardiac, renal manifestations, further complicates recognition. This patient’s overlapping DRESS and EGPA symptoms required careful clinical evaluation. Detailed chart review and comprehensive history in hypereosinophilic syndromes proved essential. The patient had over six ER visits the past year for newly diagnosed asthma, exacerbations, and rash- highlighting the importance of systemically evaluating clinical features rather than focusing on temporal association, in our case the drug exposure.
Conclusions: This case highlights the necessity of considering alternative diagnosis like EGPA in patients with persistent rash, pulmonary findings, and eosinophilia failing treatment for presumed drug reactions, and recognizing red flags such as recurrent asthma, adult-onset asthma, and sinus disease. Initiating timely immunosuppressive therapy is essential to improve outcomes. Because these syndromes require different treatments and treatment durations, timely recognition and early corticosteroid therapy expedite clinical recovery, prevent irreversible organ damage, and significantly improve patient outcomes, reduce recurrent hospital admissions, and avoid unnecessary healthcare costs.