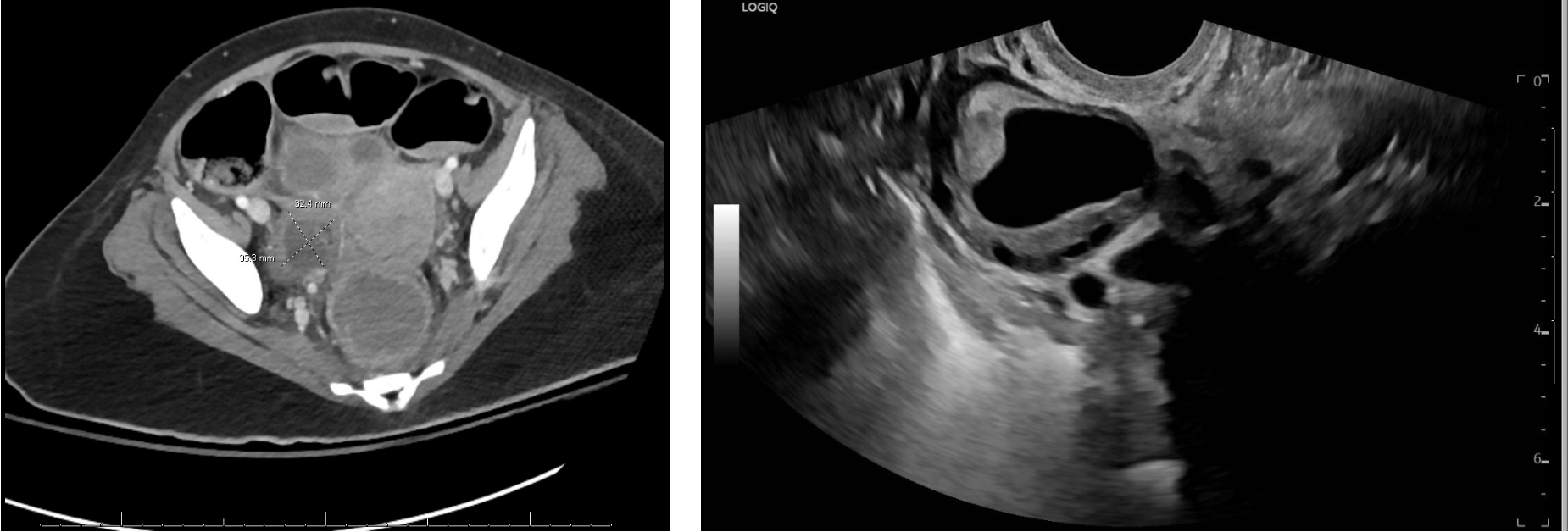
Case Presentation: A 22-year-old female with no past medical history presented to an ED with insomnia, anxiety, and hallucinations. She was given antipsychotics and admitted to a behavioral health unit on a mental health hold. Two days later, she re-presented to the ED with increased agitation requiring frequent haloperidol administration. During this visit, an LP was performed with an opening pressure elevated at 32 mmHg and CSF studies with a lymphocytic pleocytosis. MRI demonstrated only hyperintensities in the L hippocampus and insular cortex. She was treated empirically for meningitis and admitted to the hospital during which her course was complicated by seizures and required intubation, with ultimate tracheostomy, for airway protection. Her mental status continued to decline and she was unable to make purposeful movements or follow commands. Additional workup revealed a positive NMDA IgG antibody (1:640). With the diagnosis of NMDAR encephalitis made, she received plasmapheresis and corticosteroids prior to enrollment in a study protocol on hospital day seven. CT of the abdomen and pelvis on hospital day one demonstrated a “Simple right ovarian cyst measures up to 2.4 cm. Imaging evidence of a teratoma.” However, the reading of the lesion as consistent with teratoma was later rescinded and subsequent pelvic MRI on hospital day seventeen was read as a dominant right follicle without suspicion for teratoma (Figure 1). Neurologic recovery was slow and hospital course was complicated by paroxysmal sympathetic hyperactivity as well as catheter associated urinary tract infections and pyelonephritis. Additional cross-sectional imaging on hospital day thirty-six re-demonstrated “a thick-walled cystic lesion in the right adnexa” (Figure 2). At this time, transvaginal ultrasound was completed and demonstrated a “complex 3.3 cm right ovarian cystic lesion” (Figure 2). CA-125 was elevated to 57 U/mL and CEA elevated to 7.8 mcg/L. She underwent laparoscopic right salpingo-oophorectomy and removal of right ovarian mass. Pathologic examination demonstrated mature teratoma including immature neural tissue consistent with glioblastoma arising from the teratoma. The decision was made to forgo adjuvant chemotherapy in the absence of established guidelines. Following tumor resection and ongoing treatment with immunosuppressives, our patient continued to improve neurologically and is now following complex commands and able to communicate in short sentences.
Discussion: Although mature cystic teratomas (MCT) are the most common ovarian germ cell neoplasm, with 14.2 cases per 100,000 patients annually, malignant transformation accounts for only 1.5-2% of cases (1). Among malignant transformations, squamous cell carcinoma is the most common (1). Neuro-ectodermal tumors have been rarely described within mature cystic teratomas with fewer than 20 case reports (2-5). Here, we describe an additional case of malignant transformation of an MCT to glioblastoma in this young woman with NMDAR encephalitis. In this case, the ultimate diagnosis and therapeutic resection was unfortunately delayed despite multiple subsequent images due to transitions of care and ongoing motion degradation due to the underlying NMDAR encephalitis.
Conclusions: This case provides both additional evidence for the ideal management of glioblastoma arising from MCTs and highlights the necessity of a thorough investigation for a ultimate source when NMDAR encephalitis presents given its strong association with ovarian teratomas.