
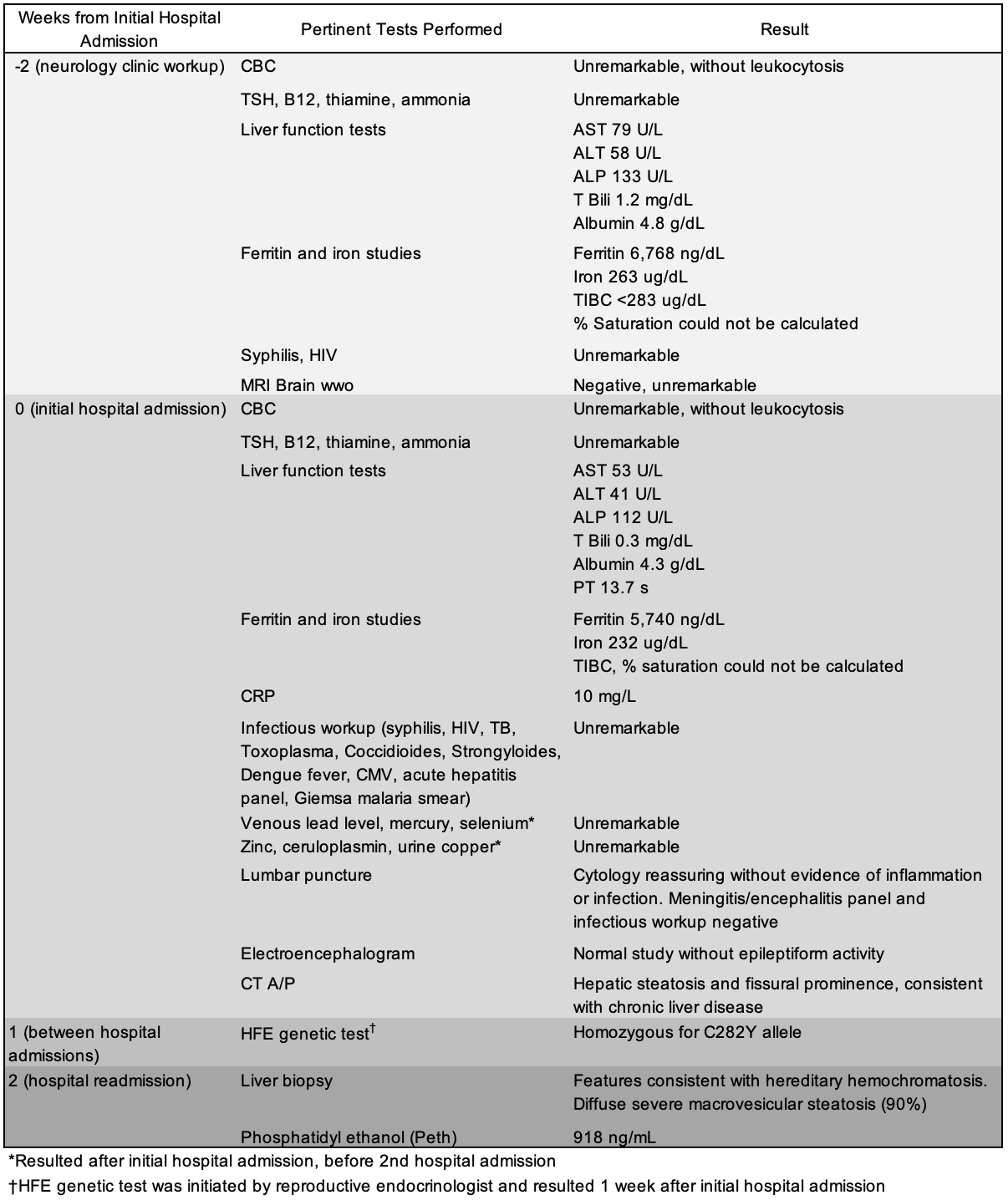
Case Presentation: A 37-year-old male (they/them) with a history of melanoma status post resection and alcohol use presented with behavioral and cognitive changes and increased falls for one year. They developed progressive fatigue, a new tremor, slowed speech, and intermittent confusion that ultimately led to a demotion at work. In neurology clinic evaluation, the team had attributed their symptoms to a psychiatric etiology after an unremarkable initial workup and neurological exam. The patient presented to the hospital two weeks later with worsened symptoms. Vital signs and physical examination were largely unremarkable. Laboratory evaluation was notable for CRP of 10 mg/L, ferritin 5,740 ng/mL, and iron 232 mcg/dL. Liver function tests demonstrated slightly elevated AST of 53 U/L and ALT of 41 U/L, with normal T Bil, PT and ALP. Neurology was consulted, and brain MRI, EEG, and lumbar puncture were unrevealing. CT A/P revealed hepatic steatosis. Given the patient’s mental status changes, elevated AST and ALT, and evidence of chronic liver disease on CT, concern was high for an underlying liver condition. Appropriate workup was initiated, and the patient was discharged with follow-up with liver and neurology teams.Approximately two weeks later, the patient was readmitted for worsening slurred speech and confusion and was found to have reduced coordination and minimal gait impairments. HFE testing revealed that the patient was homozygous for the C282Y allele, confirming the diagnosis of hereditary hemochromatosis (HH). A subsequent liver biopsy demonstrated positive iron staining and 90% macrosteatosis with an absence of fibrosis or cirrhosis.The patient began weekly phlebotomy treatment and continues to be seen by gastroenterology for their HH. They were connected with psychiatry for resources and treatment for alcohol use disorder. Now, the patient has returned to work, and all neurological symptoms have abated.
Discussion: This diagnostically challenging case illustrates an atypical presentation of HH with significant neuropsychiatric symptoms in the setting of coexisting undiagnosed alcohol use disorder. Although HH primarily presents with hepatic, endocrine, or skin manifestations, neurological symptoms may occur, particularly among male C282Y homozygotes. In fact, males homozygous for the p.C282Y HFE mutation are at almost twice the risk for dementia and delirium as males without the variant. In this case, alcohol use contributed to hepatic injury and may have played a role in the patient’s fluctuating cognitive symptoms in addition to HH. Careful, private history-taking regarding substance use is essential, and would have allowed the team to treat the patient’s alcohol use disorder earlier. Ultimately, maintaining a broad differential and searching for biological explanations for the patient’s symptoms allowed for the diagnosis of HH and alcohol use disorder, thus allowing for effective treatment that reversed their concerning symptoms.
Conclusions: This case underscores the importance of avoiding diagnostic anchoring, and of considering metabolic or hepatic causes in young adults with non-specific neuropsychiatric presentations. Neurological symptoms are unlikely to be fully explained by psychiatric illness, and thorough workup may reveal reversible biological disease.
.jpg)