Background: Tracheostomies are commonly performed for long-term airway management, but post-procedural complication rates are high, with reports ranging from 20% to over 50%.1-4 These complications require an expeditious response to reduce morbidity and mortality, but gaps in provider knowledge, training, and care delivery contribute to adverse outcomes.5 On inpatient wards, hospitalists are often the first providers responding to these emergencies. Many, however, are not routinely trained in managing tracheostomy complications and may not feel comfortable encountering them. The growing role of hospitalists in providing critical care services underscores the need for a structured curriculum targeting these gaps.6 This project introduces a novel curriculum for hospitalists using realistic simulation sessions to improve the identification and management of tracheostomy complications.
Methods: We performed a single-center, prospective study of twenty-seven hospitalists. Using a newly designed task trainer, participants underwent the following simulations: 1: Chronic tracheostomy with a cuff leak 2: Fresh tracheostomy with an occluded inner cannula 3: Fresh laryngectomy with total displacement 4: Fresh tracheostomy displacement into a false passage In the formative session, an intensivist debriefed participants after each case and discussed relevant information, differential diagnoses, and appropriate management. After a three-month interval, participants repeated the four simulations. Following each session, recordings of participants’ performances were evaluated using a standardized checklist. Changes in scores between the two sessions were analyzed with paired t-tests. Further correlations between score changes and participant characteristics, as well as their subjective ratings of the experience on a 5-point Likert scale, were analyzed with Pearson correlation.
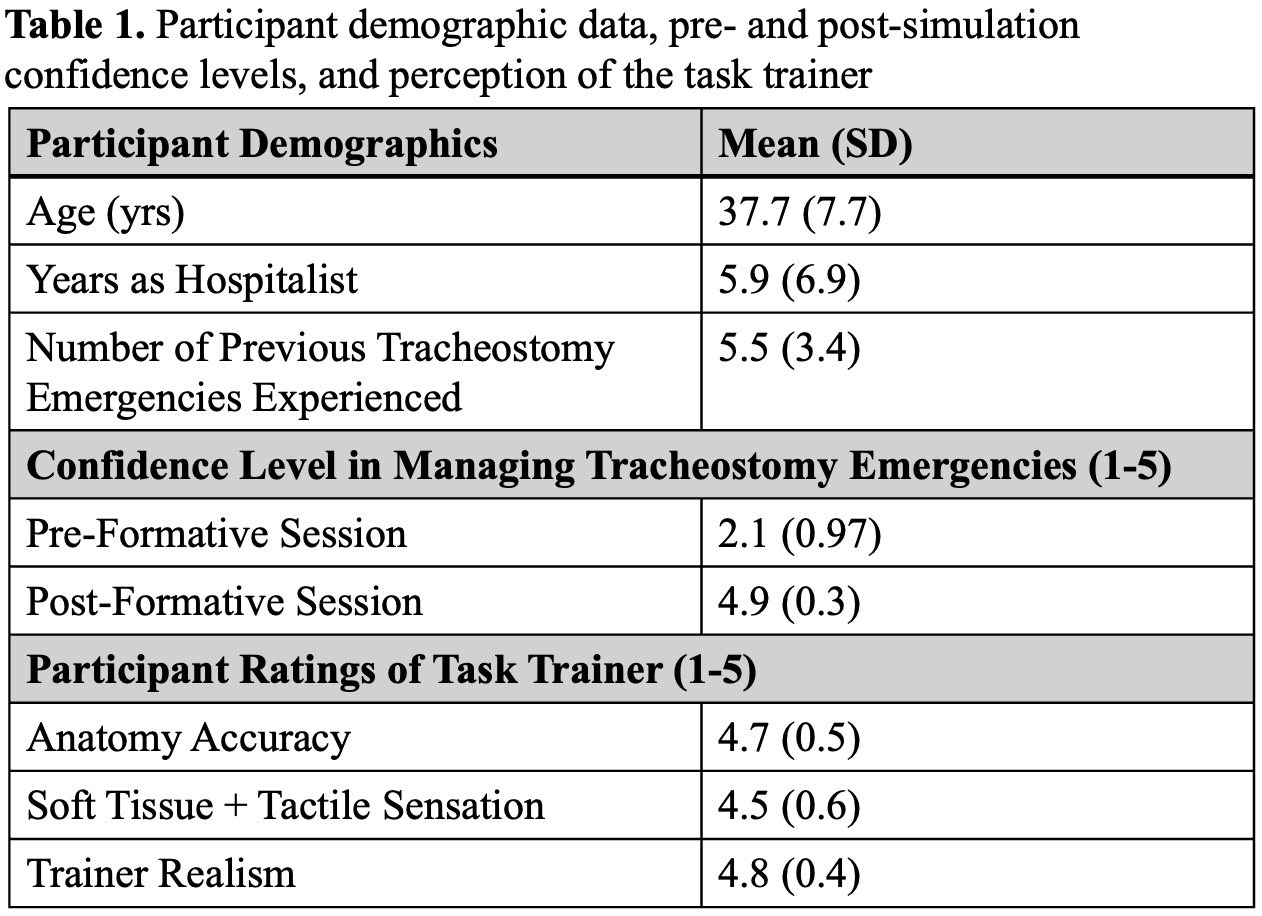
Results: Complete data, including scores, population characteristics, and survey results, were obtained for 20/27 (74%) subjects who enrolled in the study. Prior to the simulations, participants reported low confidence in their abilities to evaluate and manage tracheostomy emergencies (2.1/5). Following the formative session, participants reported high ratings (4.5+/5) in their confidence assessing and managing tracheostomy emergencies, and task trainer fidelity to real-life scenarios. Overall performances on the four cases increased from 52% (SD 22%) to 69% (SD 13%) between the two sessions (p < 0.001). Scores significantly increased for Simulations 1, 2, and 3 (p-values: < 0.0001, < 0.05, and < 0.01, respectively) but decreased, insignificantly, in Simulation 4 (p = 0.08). Number of years as a hospitalist, prior experience with tracheostomy emergencies, and subjective ratings of the simulations (usefulness, anatomy accuracy, post-training confidence level) showed no significant correlation with score change.
Conclusions: Tracheostomy emergencies require swift management by providers. Offering education and training opportunities to hospitalists who care for tracheostomy patients is one way to improve outcomes during these emergencies. Using a novel task trainer to simulate tracheostomy emergencies followed by debriefing with an intensivist, hospitalists in this study improved their overall confidence and competency in managing these scenarios. We believe this simulation-based curriculum provides a generalizable model for preparing hospitalists to manage tracheostomy emergencies.
.jpg)