Case Presentation: A 69-year-old woman presented with three days of progressive dyspnea on exertion and pedal edema. She was admitted to the hospital for an acute decompensated heart failure exacerbation. She had a history of non-ischemic dilated cardiomyopathy with severe biventricular systolic dysfunction and bilateral carpal tunnel syndrome, both diagnosed two years prior. At that time, cardiac MRI revealed possible infiltrative cardiomyopathy. Fat pad biopsy was not consistent with amyloidosis and serum and urine protein electrophoresis returned normal. She was subsequently referred to rheumatology for sarcoidosis evaluation and followed regularly in cardiology clinic. Over the past year, she had multiple hospitalizations for decompensated heart failure exacerbations despite optimal heart failure therapy.
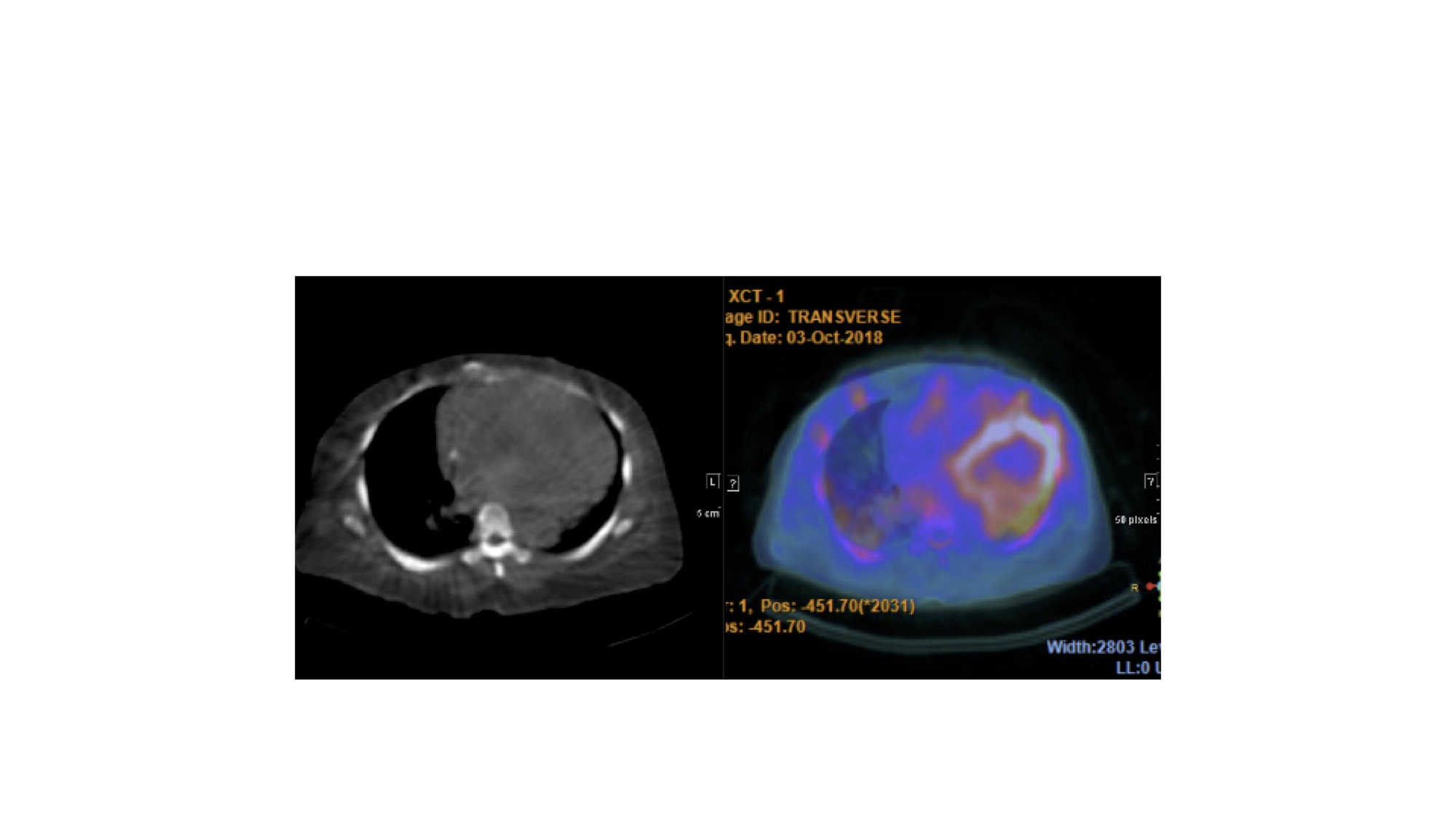
During this hospitalization, cardiac technetium-99m pyrophosphate (Tc-99m PYP) scintigraphy demonstrated an elevated heart-to-contralateral lung ratio (1.4) and heterogeneous diffuse myocardial uptake that was greater than rib uptake (Image 1). These findings were strongly suggestive of transthyretin amyloid cardiomyopathy (ATTR-CM). Despite aggressive diuresis, she continued to clinically decompensate with progressive dyspnea, hypoxia, and renal dysfunction. As investigational therapies were not available at that time, she was offered hospice but declined despite understanding her poor prognosis. Genetic testing for mutations of the transthyretin gene was offered to the patient and her family.
Discussion: Infiltrative cardiomyopathy can offer mimic hypertensive cardiomyopathy and can go undiagnosed. Causes of infiltrative cardiomyopathy include sarcoidosis, hemochromatosis and amyloidosis. Amyloid heart disease may occur due to deposition of five different proteins including thransthyretin (ATTR).
Cardiac amyloidosis due to immunoglobulin light chain deposition (AL) and ATTR-CM are often difficult to distinguish, as their clinical symptoms may be similar as well as their findings on echocardiography and cardiac MRI. ATTR-CM tends to be more slowly progressive and has a better prognosis than AL cardiac amyloidosis. ATTR-CM is often associated with carpal tunnel syndrome, which precedes heart failure symptoms more than 40 percent of the time. Unique to AL amyloid is proteinuria, macroglossia and gastrointestinal dysfunction. Definitive diagnosis is typically achieved with myocardial biopsy as the fat pad biopsy often has low sensitivity. Non-invasive diagnostic options include Tc-99 m PYP scintigraphy. This testing has 97 percent sensitivity for distinguishing ATTR-CM from AL cardiac amyloidosis. With the arrival of several emerging treatment strategies for ATTR-CM, early diagnosis is critical.
Conclusions: This case illustrates the importance of high clinical suspicion for ATTR-CM. Tc-99m PYP scintigraphy is a highly sensitive non-invasive tool for diagnosing ATTR-CM when AL cardiac amyloidosis has been ruled out.