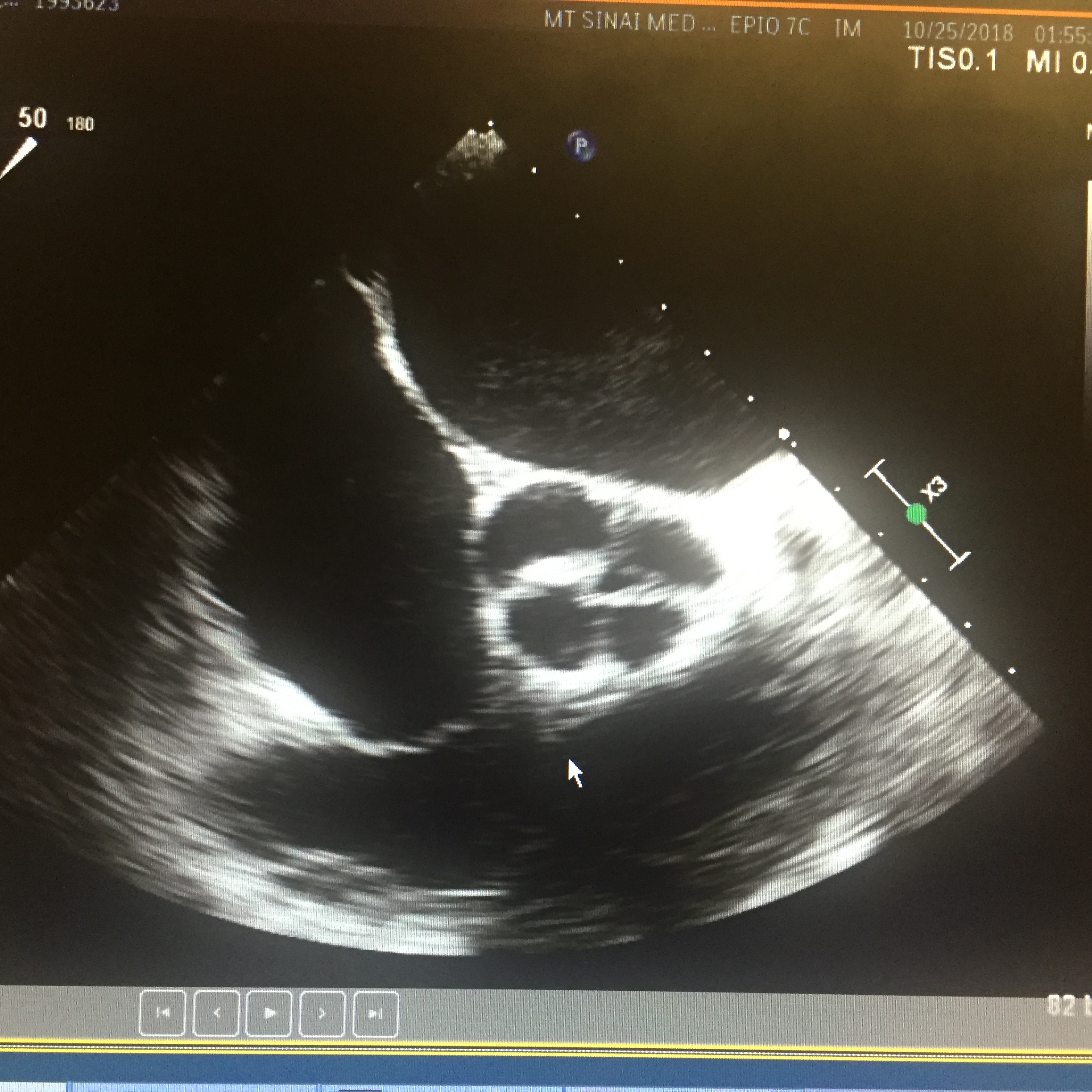
Case Presentation: A 49-year-old male presented with progressive lower extremity edema, exertional dyspnea and orthopnea for three weeks. Past medical history significant for non-ischemic cardiomyopathy, systolic heart failure and moderate aortic regurgitation (AR) diagnosed one year ago. Physical exam was significant for jugular vein distention, bibasilar crackles, loud 3/6 diastolic murmur in the aortic area with bilateral lower extremities edema. Chest x-ray revealed pulmonary congestion. Transthoracic echo showed worsening of his existing left ventricular ejection fraction (LVEF) from 30-35% one year before to 25-20%, global hypokinesis, and worsening AR. In an effort to further explain his rapid progressing heart failure and AR, the patient underwent transesophageal echo (TEE) and coronary angiogram after finishing his treatment for acutely decompensated heart failure. TEE revealed quadricuspid aortic valves with partial fusion of leaflets resulting in functionally bicuspid valve with incomplete coaptation of the leaflets with a resultant central gap. Aorta was mildly dilated measuring 4.1 cm at the level of ascending aorta. Coronary angiogram showed non-obstructive coronary arteries without anomalies. The patient is then referred for surgical aortic valve replacement and is currently waiting for surgical aortic valve replacement.
Discussion: Quadricuspid aortic valve (QAV) is a rare congenital heart defect with an incidence of 0.006%-0.033%. It usually appears as an isolated cardiac defect or less commonly in association with other congenital heart abnormalities. QAV can be asymptomatic or presented with dyspnea, chest pain, fatigue, peripheral edema or syncope. Aortic regurgitation is the predominant hemodynamic abnormality while aortic stenosis is rare.The physician should always keep a broad deferential for patients presented with recurrent heart failure exacerbation, rapidly progressing heart failure or valvular disease. Transthoracic echo (TTE) might miss some of the congenital anomalies which can presented an accelerated decline in the heart or valve function. QAV is a rare congenital defect with a diverse clinical manifestation that is usually detected incidentally in the fifth decade of life. Although the majority of cases presented as an isolated defect; many cases presented with different associated anomalies especially coronary artery anomalies which have been reported in 10% of cases. It is imperative to diagnose these associated anomalies before repair or replacement of aortic valve to avoid ostial obstruction.
Conclusions: The physicians should be aware of the possibility of abnormal valve structure in any case of aortic regurgitation with newly onset heart failure especially in the absence of the well known risk factors. Although transthoracic echo (TTE) can detect most cases, some cases may need TEE to reach the diagnosis. Patients with QAV are at higher risk of endocarditis associated with QAV in comparison to the normal aortic valve; however, antibiotics prophylaxis is not indicated. Surgical repair carries an excellent prognosis.