Case Presentation: Severe peripheral disease with arterial thrombosis can present as bilateral leg paralysis and extreme pain. Caution must be exercised to exclude vascular pathology ( in addition to neurologic differentials), to avoid premature closure of diagnosis and to avoid catastrophic outcomes. One such rare disorder is Leriche syndrome, whereby, patients develop aortoiliac thrombotic occlusion, compromising lower extremity perfusion.
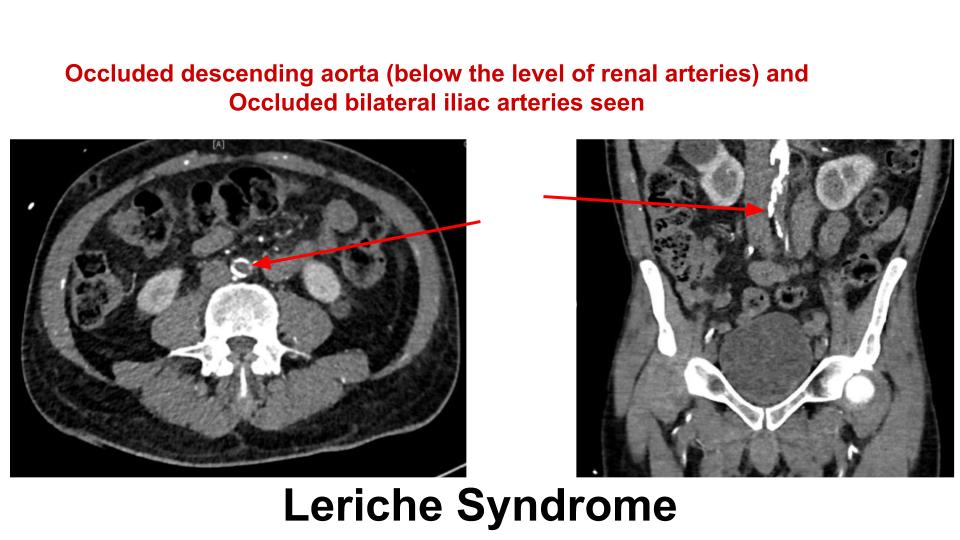
65-year-old man with chronic tobacco smoking disorder, poorly controlled diabetes mellitus, HFrEF, CAD, pulmonary hypertension, chronic claudication, and erectile dysfunction presented to ED with worsening bilateral leg pain and difficulty ambulation. Patient lives at home alone, doesn’t care well for himself and continues to smoke cigarettes. He has been experiencing erectile dysfunction and bilateral leg pain for a few months, but for the last few days, both pain and leg weakness got worse to the point that he was unable to bear weight on legs and walk. Initially, he was thought to have spinal cord compression pathology, but given his pain, a contrast CT of abdomen and lower extremities was requested, which showed aortoiliac occlusive disease (Leriche Syndrome). He was also found to have a coexisting DVT of left popliteal vein, but May-Thurner Syndrome was ruled out with normal iliac vein. This was considered an emergency, he was started on heparin infusion and vascular surgery was consulted. Additionally, his CPK level was 29000 and lactate was high. No evidence of acute compartment syndrome was found, but given his overall clinical condition and rhabdomyolysis, patient was recommended surgical intervention. Unfortunately, due to symptomatic CAD, surgery was delayed – he underwent PCI and drug eluting stent placement in LAD, following which, he underwent left above knee amputation and right axillofemoral bypass surgery. He was started on dual antiplatelet therapy (Clopidogrel, Aspirin) as well as coumadin for severe PVD and DVT. He was discharged to rehabilitation and has been slowly recovering, and maintaining close follow up with primary care doctors.
Discussion: Leriche syndrome (AIOD) is chronic thrombotic occlusive disease of abdominal aorta immediately above bifurcation site, presenting with triad of leg claudication, erectile dysfunction and absent femoral pulses. Causes include hypercoagulable state (genetic or acquired such as contraceptives, cancer, tobacco etc), surgery, trauma, atrial fibrillation, aneurysms etc. Obesity, hypertension, diabetes mellitus, dyslipidemia, and smoking are leading risk factors. TASC II classifies AIOD as a type D lesion, with surgery as the recommended management (aortobifemoral bypass grafting/ABF, although in some cases axillo-bifemoral or a unilateral axillo-femoral/aorto-femoral bypass may be used). Even with surgery, morbidity burden remains high.
May Thurner Syndrome is compression of left common iliac vein by right common iliac artery causing a DVT, which was ruled out in this patient. May-Thurner syndrome has been reported in Leriche syndrome case, hence one should be mindful of such association. More cases need to be reported to understand if, in fact, there is such an association.
Conclusions: This patient had many risk factors such as DM, Dyslipidemia, obesity, smoking, that caused AIOD. He is counseled to abstain from smoking and continue with medication adherence. Despite efforts, this patient’s left leg could not be salvaged but underwent right leg bypass.