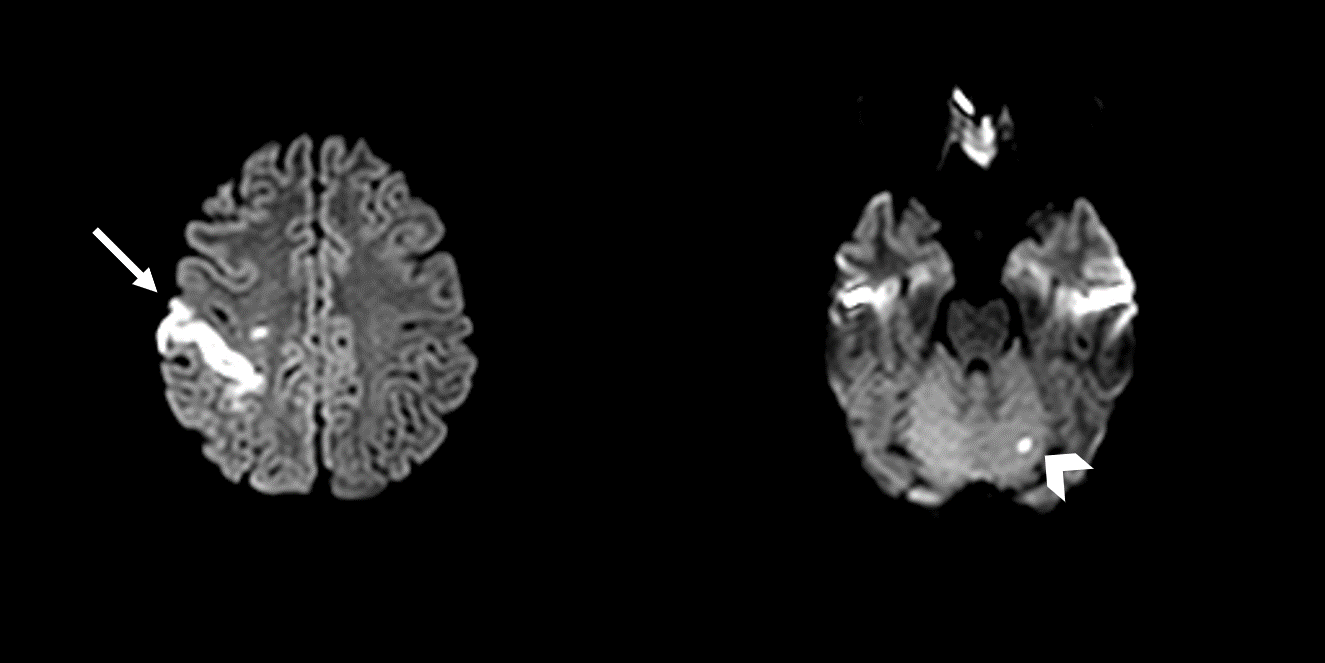
Case Presentation: An 8-week pregnant G5P1041 24-year-old African American female with no past medical history presented with acute onset left-sided weakness, slurred speech, and paresthesia. Her symptoms started a day after taking one dose of misoprostol as morning-after pill. She used misoprostol multiple times previously with neither neurological nor cardiovascular symptoms. On physical examination, her vitals were unremarkable. She had decreased touch and temperature sensations involving the left cranial nerve V2 territory and left side of her body. She also had weakness in her left distal upper extremity involving the wrist and digits. Strength was otherwise normal. Her blood work included a positive human chorionic gonadotropin of 93,981.6 milli-international units per milliliter, mild hyperlipidemia with a low-density lipoprotein of 133 milligrams per deciliter, unremarkable factor II, factor V, and lupus anticoagulant tests. Electrocardiogram, transthoracic and transesophageal echocardiograms were all unremarkable. Magnetic resonance imaging (MRI) of the brain without contrast showed evidence of ischemic infarcts involving the right frontoparietal region (middle cerebral artery territory) and left cerebellum. Head and neck magnetic resonance angiography was non-significant for any intracranial or extracranial artery stenosis. During her 6-day hospital course, her left-sided weakness and fine motor movements improved. She continued to have mild left-sided residual sensation loss compared to the right side. She was discharged with a loop recorder and monitored for five days without significant findings.
Discussion: Misoprostol, a synthetic prostaglandin E1 (PGE1) analog, is a cost-effective medication commonly used for elective abortion during the first trimester (1,2). However, various case reports identified adverse effects even in healthy young women after misoprostol use, including strokes, transient acute coronary artery vasospasm, and myocardial infarctions (3,4,5,6,7). We report a rare case of a cryptogenic stroke in a healthy, young female after one dose of misoprostol administration. Although prostaglandin effects of vasodilation and inhibition of platelet aggregation should theoretically counteract stroke, there have been studies showing possible low-dose vascular vasoconstriction and high-dose vasodilation (8.9.10,11,12). Alternatively, prostaglandins can bind to prostaglandin EP3 receptors in the brain, triggering calcium channels, and ultimately inducing cerebral ischemia (4,13,14). Both methods together are suspected to be the etiology for how misoprostol can cause ischemic strokes. In our patient, cardioembolic cause was unlikely in the setting of negative echocardiograms. Besides, her negative hypercoagulable workup and multi vascular territory affection on the MRI made thrombotic causes unlikely as well. In the setting of these givens, we highly suspect that misoprostol was the causative agent of her stroke.
Conclusions: Misoprostol is a commonly used medication for elective abortion, however, there is increasing evidence of adverse cardiovascular and cerebrovascular events associated with its use. Currently, no treatment options are available for such events. Further research is required to characterize the prevalence of these adverse events, especially in patients with vascular or hematological risk factors. Until then, cautious use of misoprostol and vigilance to its adverse events are warranted.