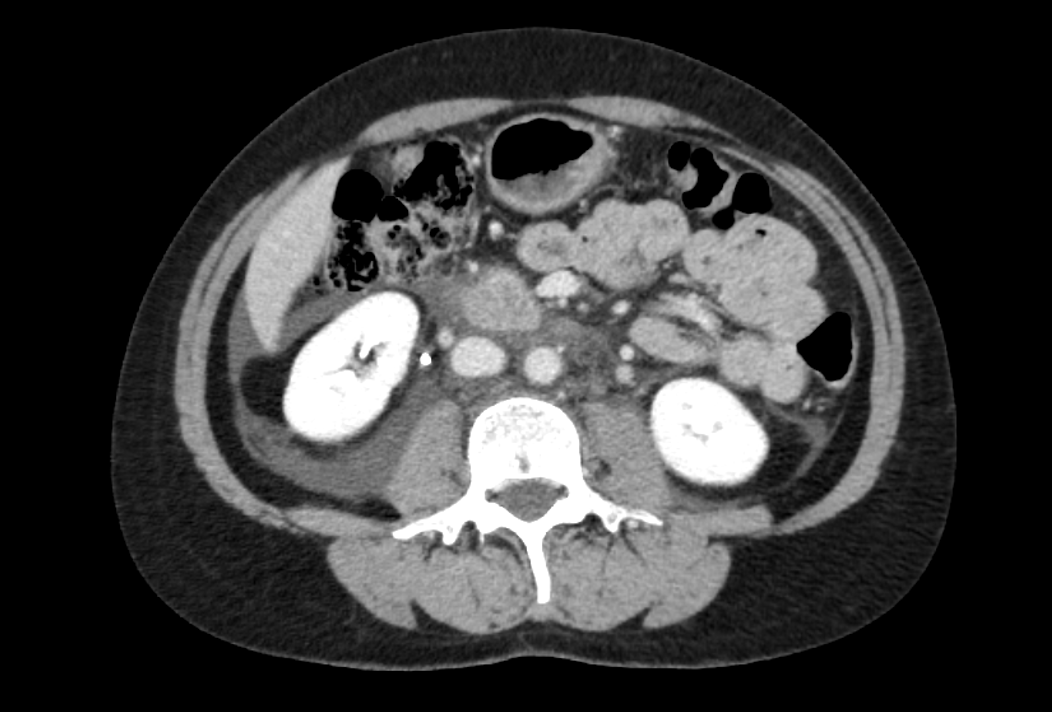
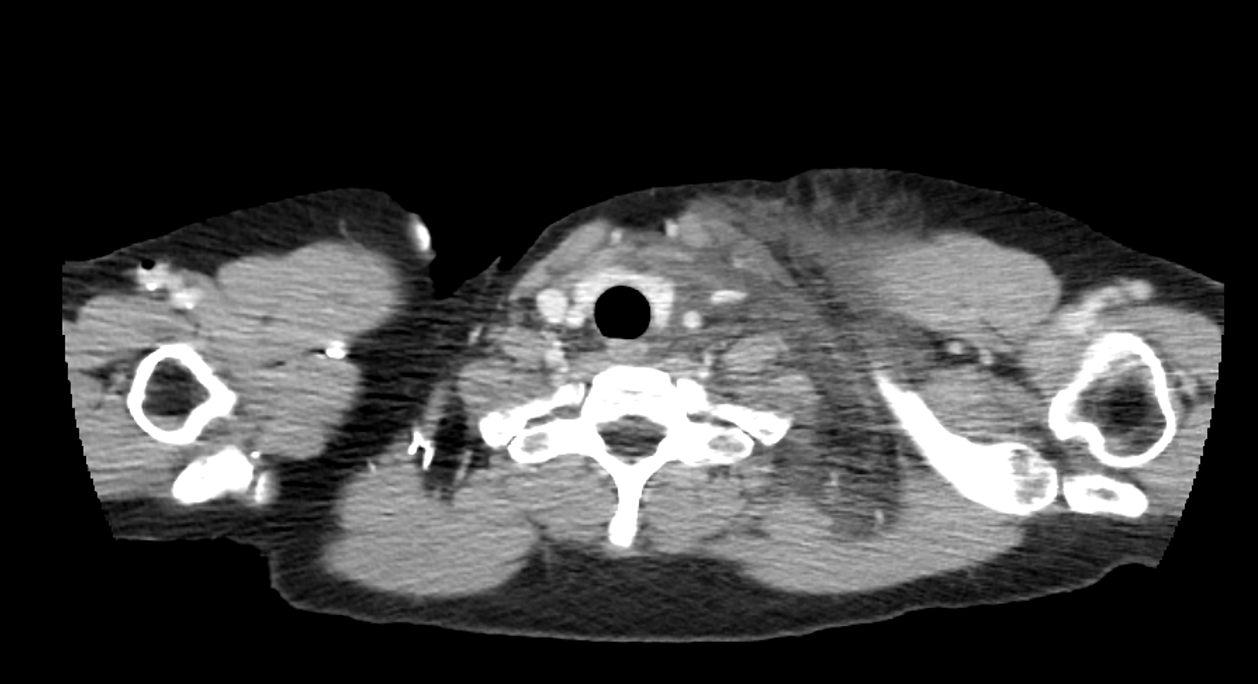
Case Presentation: A 46-year-old woman experienced difficulty swallowing while drinking coffee in the evening of her visit. Shortly afterward, she developed rapid swelling in the left neck region, accompanied by syncope, and was transported to a local hospital for emergency care. Blood tests and electrocardiography showed no abnormalities. However, a CT scan revealed swelling of the soft tissues extending from the left neck to the anterior chest wall and mediastinum. In addition, blurred fat tissue was observed in the periaortic and pericaval regions of the abdomen, the retrorenal space, and the retroperitoneal area, including the broad ligament of the uterus.The patient continued to experience episodes of syncope after arrival, leading to hospitalization. However, the swelling in her left neck subsided within a few hours and completely resolved by the following morning. She was subsequently referred to our outpatient clinic for further investigation. Follow-up CT scans showed resolution of all previously identified abnormalities. The activity of C1 inhibitor was normal, ruling out hereditary angioedema. Despite extensive investigations, no definitive cause was identified, and observation was continued.Fifty-three days later, she experienced sudden swelling in her right elbow and a sensation of throat tightness. Both symptoms resolved within a few hours. Detailed questioning revealed that she had taken zolmitriptan before the onset of symptoms in both episodes. Based on existing reports of triptan-induced angioedema, the patient was diagnosed with angioedema caused by zolmitriptan.
Discussion: Although this case presented with atypical symptoms, including swelling of the left neck and retroperitoneal regions, the sudden onset of localized swelling that resolved spontaneously suggested the possibility of angioedema. However, the exact cause could not be determined at the initial evaluation. C1 inhibitor activity was normal, and this being the first episode, hereditary angioedema was ruled out. Additionally, the absence of a history of ACE inhibitors or NSAIDs, which are common causes of drug-induced angioedema, led to the erroneous conclusion that the condition was not drug-related.Two factors contributed to the delayed diagnosis in this case. First, the patient had been receiving treatment for migraines at another clinic but had not informed healthcare providers about her use of triptans as a rescue medication. The delayed onset of symptoms, occurring several hours after zolmitriptan administration, also likely prevented the patient from associating the drug with her symptoms.Second, reports of triptans causing angioedema are extremely rare and are not widely recognized among physicians. As a result, neither the referring physician nor the primary care physician thoroughly inquired about her history of triptan use.Nevertheless, even without prior knowledge of the association between triptans and angioedema, obtaining an accurate history of zolmitriptan use could have prompted a review of adverse event reports and led to an earlier diagnosis. This case underscores the critical importance of obtaining a comprehensive medication history, including as-needed medications, as part of clinical reasoning.
Conclusions: Triptans can potentially cause angioedema. Comprehensive history-taking, including as-needed medications, is essential in identifying the cause of angioedema.