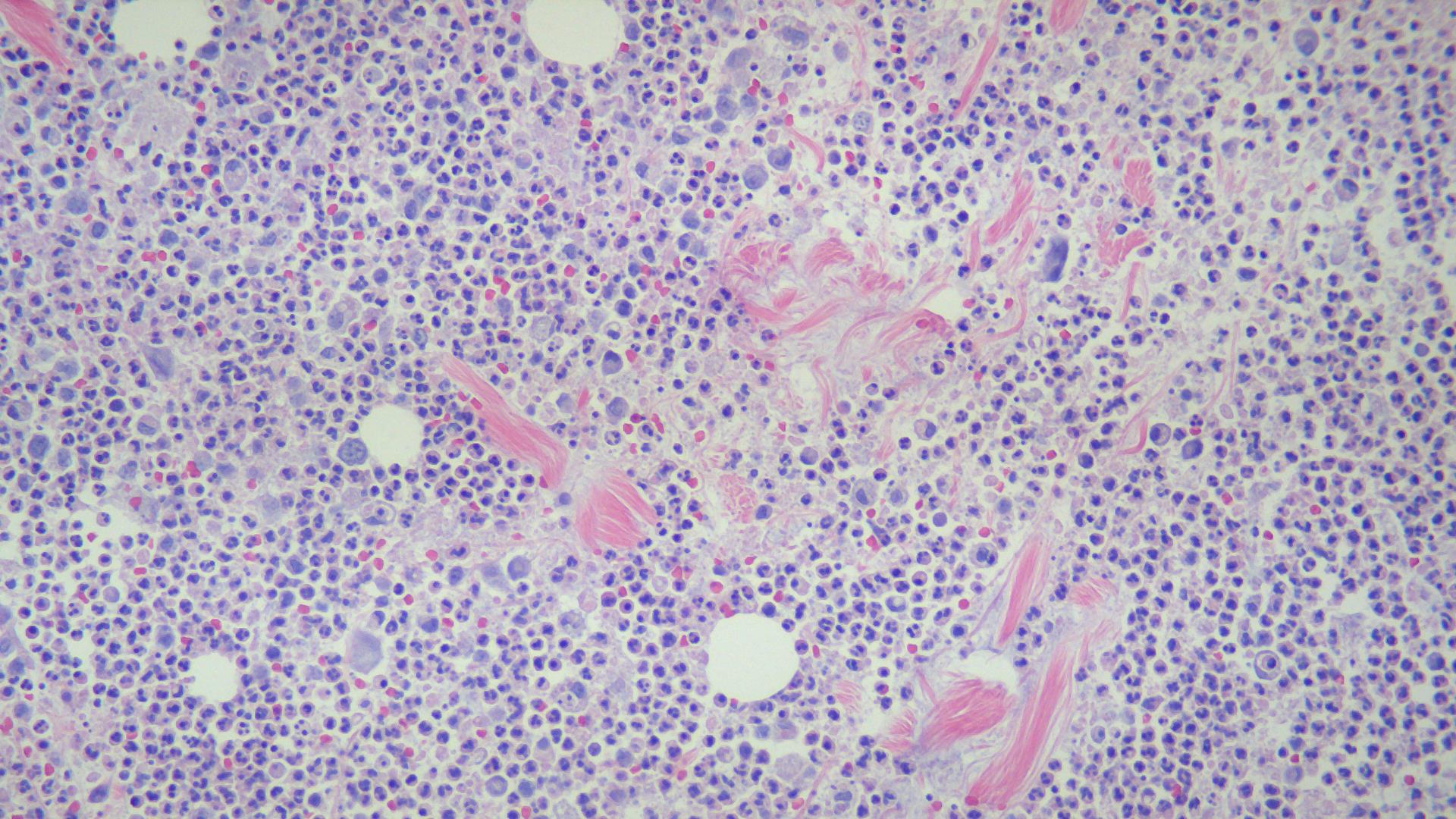
Case Presentation: 35-year-old Caucasian gentleman who was diagnosed with alpha-1 antitrypsin deficiency (PiZZ) 2 years ago. Two weeks prior to the hospitalization, he noticed skin nodules on both sides of the abdominal wall and in the upper thighs. He also noticed a lesion that looked like a boil on his right shin, started draining and gradually the redness extended over to the right ankle. CT scan of the right foot and ankle revealed extensive soft tissue edema in the ankle and foot with multiple pockets of fluid collection raising the suspicion for an abscess. The right foot wound was debrided but all cultures came back as negative for bacterial growth. ANA/ANCA/Rheumatoid factor screen was negative. Excision biopsy of a large right medial thigh lesion is done, and pathology revealed necrotizing lobular panniculitis with neutrophils, lymphocytes and histiocytes consistent with alpha-1 antitrypsin deficiency. He is treated with intravenous alpha 1 antitrypsin infusion, dapsone and prednisone resulting in significant improvement of the skin lesions
Discussion: Alpha-1 antitrypsin panniculitis is an inherited disorder characterized by low serum alpha 1 antitrypsin levels. It presents as recurrent, tender, erythematous plaques or nodules with a tendency to ulcerate on the trunk, buttocks and proximal extremities. The lesions may be precipitated by trauma. Deep incisional biopsy and review of the pathology might help pinpoint the diagnosis. Histology will reveal predominantly lobular panniculitis without vasculitis. (Differential Diagnosis- In erythema nodosum it is septal panniculitis without vasculitis. Cutaneous polyarteritis nodosum- septal panniculitis with vasculitis). Treatment options include intravenous pooled human plasma alpha 1 antitrypsin infusion, plasma exchange, dapsone, steroids and liver transplant.
Conclusions: Alpha 1 antitrypsin deficiency panniculitis is an under recognized condition. Prompt diagnosis may result in treatment with intravenous pooled human plasma alpha-1 antitrypsin that can result in rapid improvement.