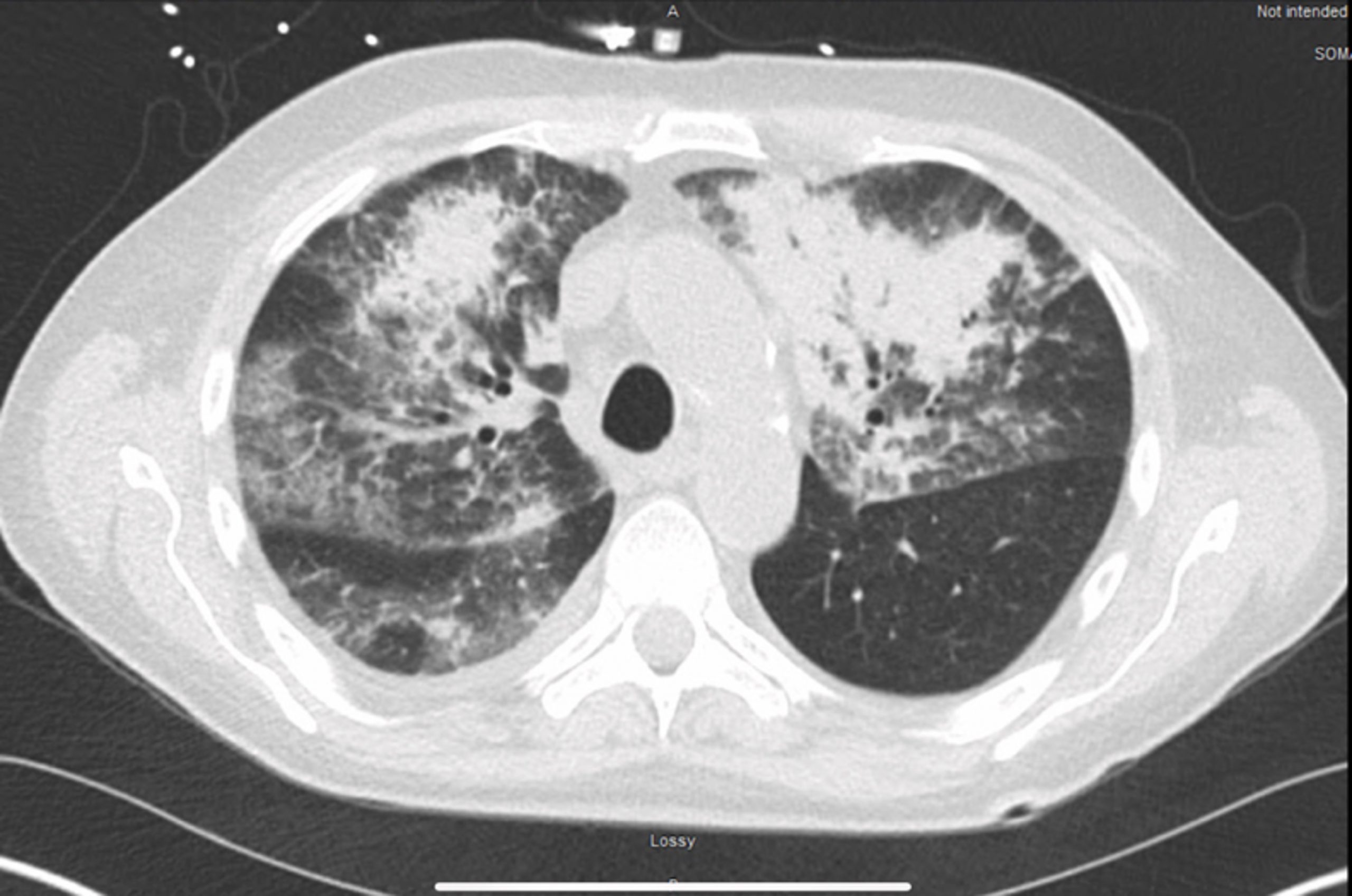
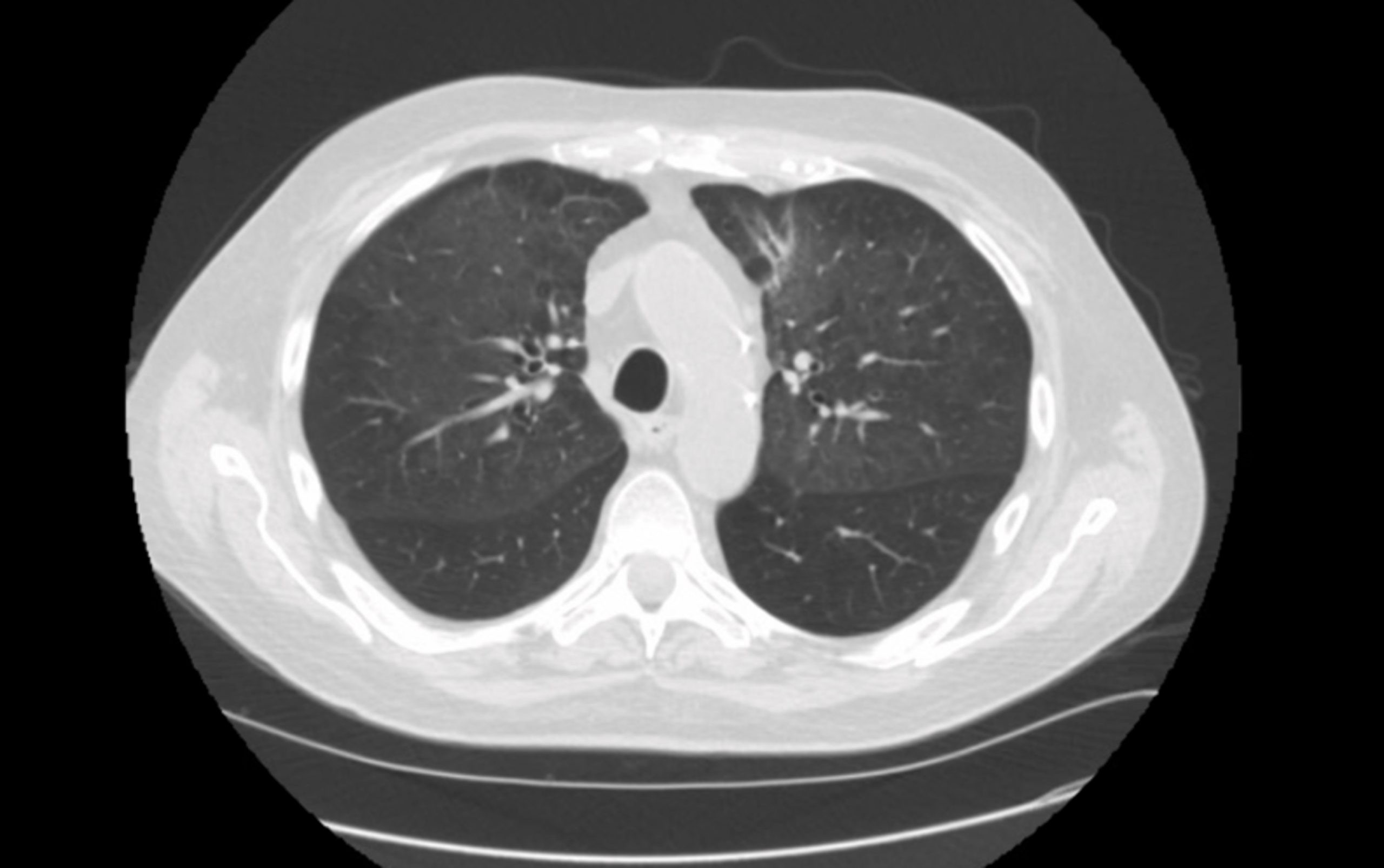
Case Presentation: A 71 years old white male, with a past medical history of severe eosinophilic asthma, was transferred to our hospital with hypoxemic respiratory failure and worsening infiltrates. Respiratory PCR was negative. The patient was febrile with T-max of 101 F, required 6 L of oxygen. Labs showed WBC 21,000, Hemoglobin was7.4, and Creatinine was 1.4. Repeat respiratory PCR was positive for Influenza A, COVID 19 was negative. The patient’s clinical condition and labs improved with Oseltamivir, Vancomycin, and Cefepime and oxygen requirement improved to 2 L. Within a few days, he deteriorated, developing a non-blanching rash on both lower extremities and hemoptysis. Renal function declined (Cr from 1.0 to 3.5) along with the progression of anemia and hypoxemia, requiring 5L of oxygen. UA showed 150 RBC, 2+ proteins and spot UPC of 1.73. CT chest showed new bilateral ground glass pulmonary infiltrates. Further workup showed positive ANCA serology >1:640, with anti-MPO Ab >100. A clinical diagnosis of ANCA vasculitis associated with Influenza-A, was established. The patient was started on induction therapy with pulse dose steroids and Cytoxan. Plasma exchange was not considered in light of the PEXIVAS trial, which did not show benefit on survival. Upon 6 weeks follow up, the patient improved. He maintained oxygen saturation in the 90s on room air with Creatinine improved to 1.4. Repeat CT chest showed almost complete resolution of the infiltrates. Repeat serology improved with c-ANCA Titer <1_20 and anti-MPO Ab <9.
Discussion: ANCA associated vasculitis is a rare (1/20 million) small-vessel necrotizing vasculitis associated with ANCA, specific for either MPO or PR3, which involves multiple systems, especially lungs and kidneys. The pathogenesis is multifactorial and influenced by genetics, environmental factors, and the response of the innate and adaptive immune system. The mechanism involves ANCA-mediated excessive activation of neutrophils that subsequently release cytokines, reactive oxygen species and lytic enzymes. Bacterial infections have been thought to be an important factor in the initiation of this mechanism. ANCA associated vasculitis is a reported complication of Influenza Vaccine. One case has been reported regarding Influenza A-induced ANCA vasculitis with an elevated titer of anti-PR3. This would be the first case of Influenza A-induced vasculitis with elevated anti-MPO titer.
Conclusions: We postulate that, Influenza A infection might play a role via molecular mimicry in developing autoantibodies against the host immune response system, leading to ANCA vasculitis.