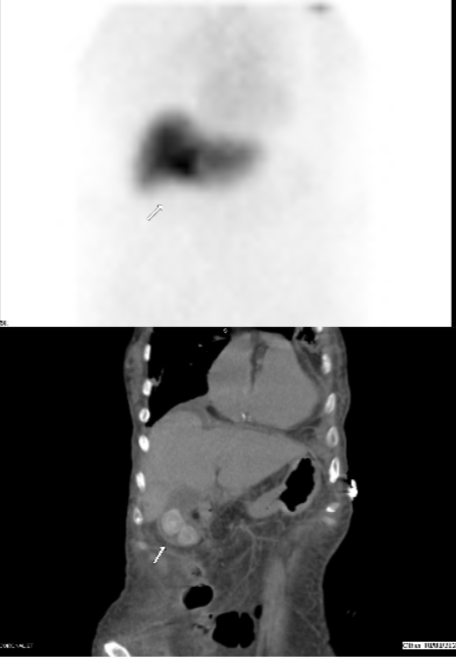
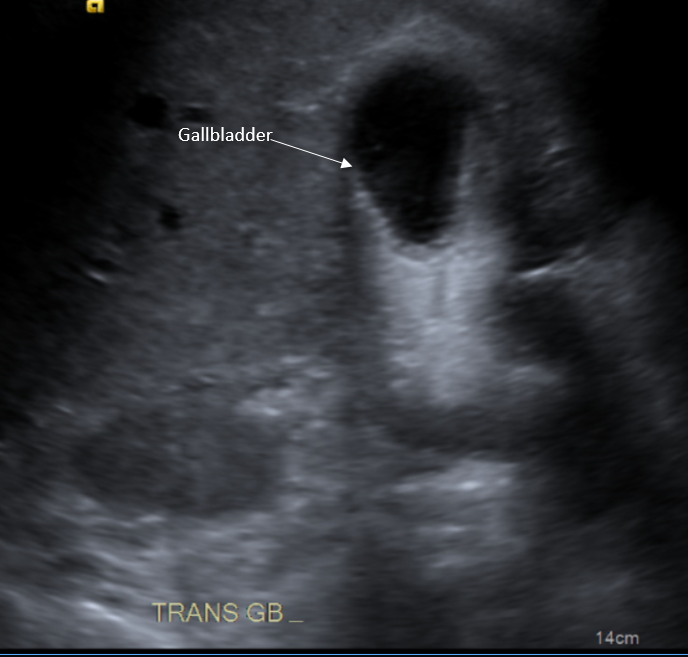
Case Presentation: An 86-year-old female with advanced dementia presented with a four-day history of worsening encephalopathy and jaundice with associated severely poor oral intake. The patient had progressive weakness, increased work of breathing, and vague abdominal pain. The initial exam demonstrated lower abdominal tenderness to palpation with guarding. She was admitted for septic shock requiring the administration of multiple vasopressors. The patient’s hyperbilirubinemia and transaminitis (total bilirubin 7.8 mg/dL, AST 292 IU/L, ALT 423 IU/L, ALP 62 IU/L) were consistent with a mixed hepatocellular-cholestatic pattern of injury and the patient was empirically started on ciprofloxacin and metronidazole. An ultrasound depicted cholelithiasis and a thickened gallbladder wall. A subsequent HIDA scan showed no radiotracer activity in the gallbladder or small bowel, suggestive of a cystic or common bile duct obstruction with concern for acute cholecystitis with cholangitis. Given her inherent instability with concern for decompensation, cholecystectomy and ERCP/sphincterotomy were not pursued and the patient instead received a bedside cholecystostomy tube. Blood cultures grew Elizabethkingia species (spp.) so empiric sulfamethoxazole-trimethoprim was started. The source of the bacteremia was unclear, but thought to be likely secondary to acute cholangitis. Repeat blood cultures confirmed growth of Elizabethkingia spp.; however, the cholecystostomy cultures were without growth. Other sources for the cause of bacteremia including a urinalysis and a CT abdomen/pelvis were unprolific.Given the rarity of Elizabethkingia spp. bacteremia, sensitivities and precise identification of the species were unobtainable. Per discussion with the Infectious Diseases consultant and per existing evidence, there is a high response rate to minocycline and piperacillin-tazobactam and the antibiotic regimen was adjusted accordingly. Despite multiple consultants and medical interventions, her multiorgan failure progressed to include acute hypoxic respiratory failure, heart failure with reduced ejection fraction, acute renal failure, disseminated intravascular coagulation, and acute liver failure. The patient’s family elected to transition her to comfort care and she was compassionately extubated after a prolonged hospitalization.
Discussion: Limited case reports have shown Elizabethkingia spp. bacteremia presenting as nosocomial infections, particularly in immunocompromised patients. Elizabethkingia species bacteremia has a high mortality of 25-30% [1-3]. As illustrated by this case, species identification was lacking as it required sequencing not typically performed in a hospital setting [4]. Elizabethkingia spp. has shown resistance to β-lactam and carbapenems, and growing resistance to fluoroquinolones [4]. Increased awareness of Elizabethkingia spp. progresses scientific knowledge to earlier identification and a more targeted approach to treatment.
Conclusions: Due to the rarity of Elizabethkingia spp. infections, there have been limitations in research. Our case study demonstrates the unique presentation of the Elizabethkingia spp. as a highly resistant nosocomial infection with great morbidity and mortality. Early and accurate diagnosis is key to treating infected patients. More research must urgently be done to investigate characteristics, especially drug susceptibilities, of said species.