Background: The transition period from hospital to home is a critical phase in patient care. Inadequate transitions can lead to adverse events, readmissions, delays in care, increased healthcare expenses and increased morbidity and mortality. Individuals with diabetes are particularly susceptible to readmission, facing a significantly higher risk compared to those without the condition. Furthermore, diabetic patients who have concomitant health related social needs such as food insecurity and poor access to medications are almost twice as likely to be readmitted and exhibit higher rates of healthcare usage. Therefore, prioritizing interventions targeting this vulnerable patient group during pivotal transition periods is essential for delivering equitable, high-quality care.
Purpose: Our project aims to utilize existing interprofessional diabetes care teams in both inpatient and outpatient settings to facilitate optimal transitions of care (TOC) for a significantly underserved patient demographic. Our goal is to enhance health outcomes by specifically targeting reductions in HbA1c levels, alongside decreasing hospital readmissions, and enhancing access to food and medications pertinent to diabetes management.
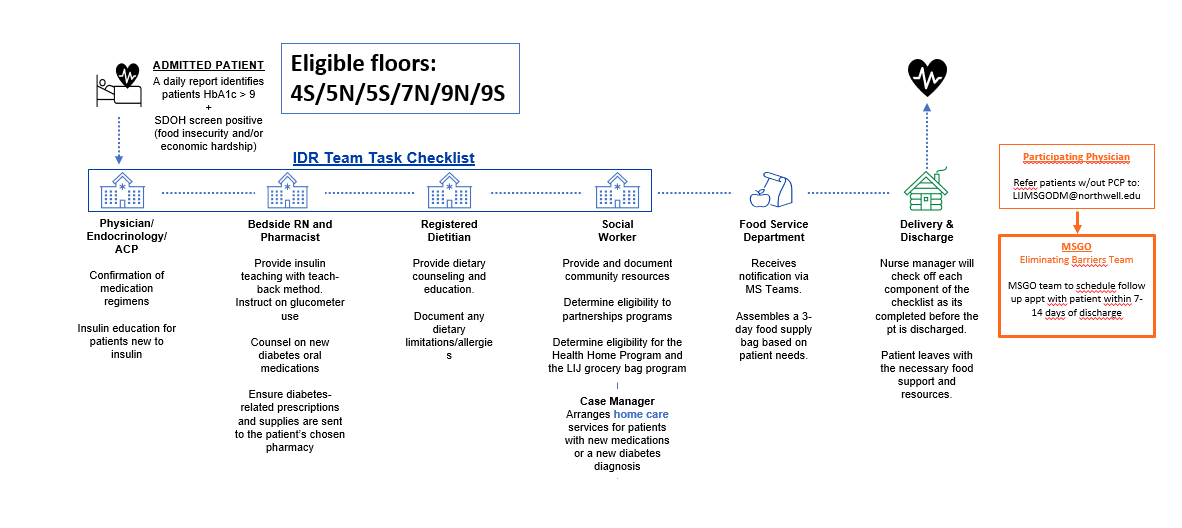
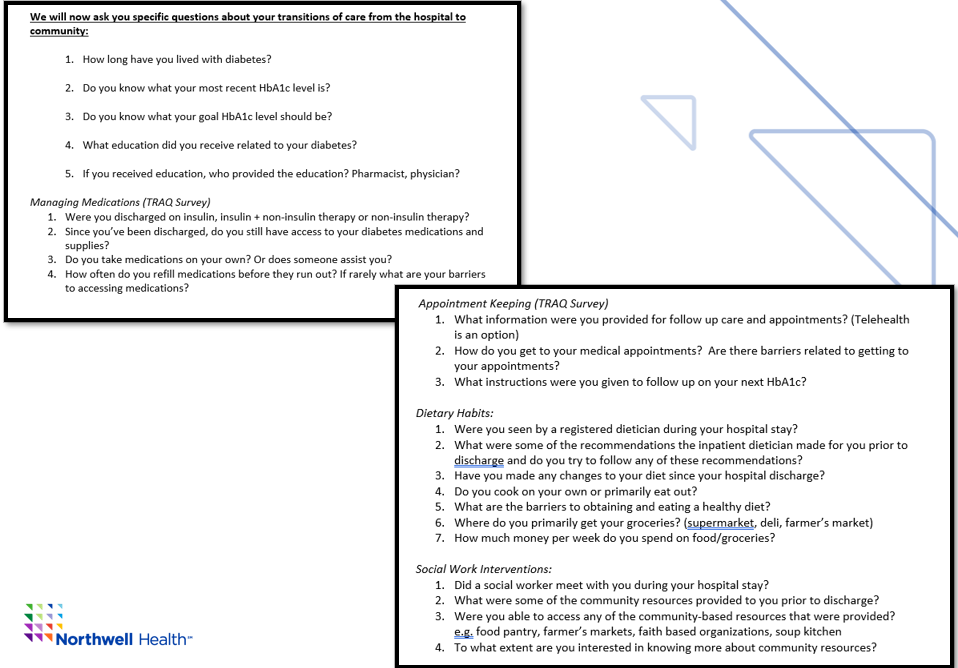
Description: We will identify all admitted patients diagnosed with any form of uncontrolled diabetes with HbA1c greater than or equal to 9 across six of our medicine/telemetry units at out site. Subsequently, we will narrow the patient cohort to include those who also screen positive for food insecurity and/or economic hardship. Following patient identification, we will trigger the inpatient transitions of care team and ensure there is a transitional handoff provided to the outpatient setting. The patient can choose to continue to follow with their own primary care doctor or we will transition the patient to our established internal medicine resident clinic (MSGO – medical specialties of Glen Oaks). At MSGO, there exists an interprofessional diabetes care team that has already proven to successfully reduce their enrolled patient population’s HbA1c by 2 points.We will conduct a 30 day post discharge phone call and ask a series of questions to the patients related to the transitions of care program. We will collect this information in a shared patient protected database to understand the impact a transitions of care team has on our underserved patient population.
Conclusions: Our outcomes will illustrate the critical need for interprofessional transitions of care teams, especially for prevalent conditions like diabetes, which greatly affect our underserved patient demographic. Success of this study will be determined by showing reduction in baseline HbA1c levels, readmissions to the hospital, visits to the emergency room, and improvement in access to healthy foods and diabetes medications. We hope to present the results of our work in future research studies.