Background: Within 3 weeks of hospital discharge, about 19% of patients experience an adverse event, with 66% of these being an adverse drug event. During a patient’s transition from hospital to home, pharmacists have identified and resolved medication discrepancies. Inappropriate continuation or discontinuation of medications post-hospital discharge often stems from medication list complexity, inconsistent or multiple pharmacy supply sources, and inaccuracy of patient self-reporting. At UC San Diego (UCSD) Health, we implemented a Hospitalist-led virtual transition of care (VToC) clinic with integrated pharmacists conducting pre-visit medication reviews with documentation of medication-specific concerns and provide real-time availability to address any concerns during the visit. VToC clinic appointment occurs ideally within 7 days post-discharge.
Purpose: -Define the role of pharmacist in the VToC clinic at UCSD Health-Report the most common VToC pharmacist interventions-Discuss the expansion of pharmacist support for all VToC patients
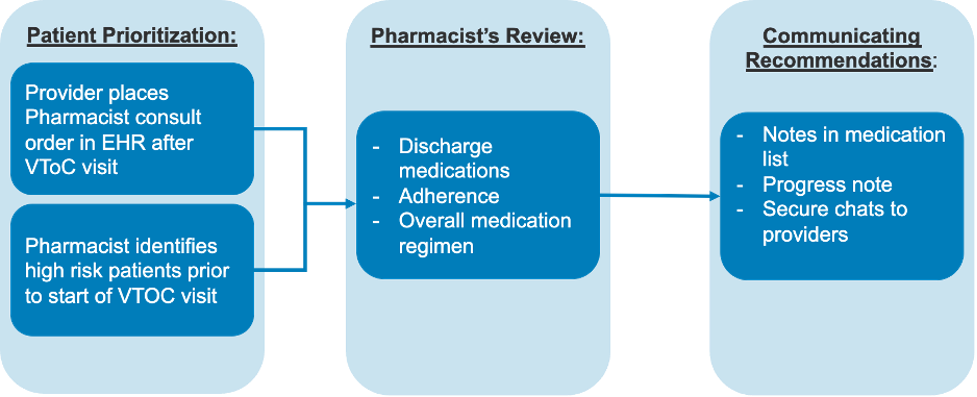
Description: Methods:VToC pharmacist support is available 8 hours per week, divided into two 4-hour days at the beginning and end of the week (workflow is in Figure 1). The pharmacist conducts pre-visit reviews of patients’ discharge and home medication lists and adherence using refill history. The pharmacist completes these prior to the appointment so that the physician will have the medication-specific concern(s) listed in the EHR’s medication list and pharmacist progress note. The pharmacist is also virtually available for physician consultations via secure messaging within the EHR or a consult order. Since not all scheduled patients can be reviewed, patients with a high UCSD-RX Risk Score are prioritized. Higher scores correlate with increased risk of 30-day unplanned readmission and likelihood of medication errors at discharge. Medication-specific concerns are relayed to the physician via notations in the medication list and in a pharmacist progress note written before the visit. An IRB-exempt, retrospective review was conducted from 1/1/2023 to 10/31/2023 of patients scheduled in VToC clinic with pharmacist involvement. Descriptive analysis of interventions was conducted categorizing types of pharmacist interventions made for each patient. Results:Baseline patient characteristics and the types of pharmacist interventions are in Table 1. The VToC pharmacist reviewed 331 out of 751 patient visits scheduled (44%). 71% of these patients required an intervention, with updating home medications and coordinating drug access being the most frequent. Other interventions included adjusting medication dose or frequency and preventing and managing adverse drug events and drug-drug interactions. Patients with medications sent to the internal hospital discharge pharmacy had fewer medication access issues than prescriptions sent to an outside pharmacy (19% vs 22%).
Conclusions: VToC pharmacists play a key role in patient safety by facilitating medication reconciliation after a patient’s hospital discharge. For Hospitalists overseeing the discharge process, the VToC team provides education on best practices, such as sending prescriptions to the internal discharge pharmacy, assessing patient’s needs for medication refills, and ensuring the accuracy of the discharge medication list. Future goals of VToC clinic include expanding pharmacist support to ensure all scheduled patients have pre-visit medication reviews and pharmacist consultation.