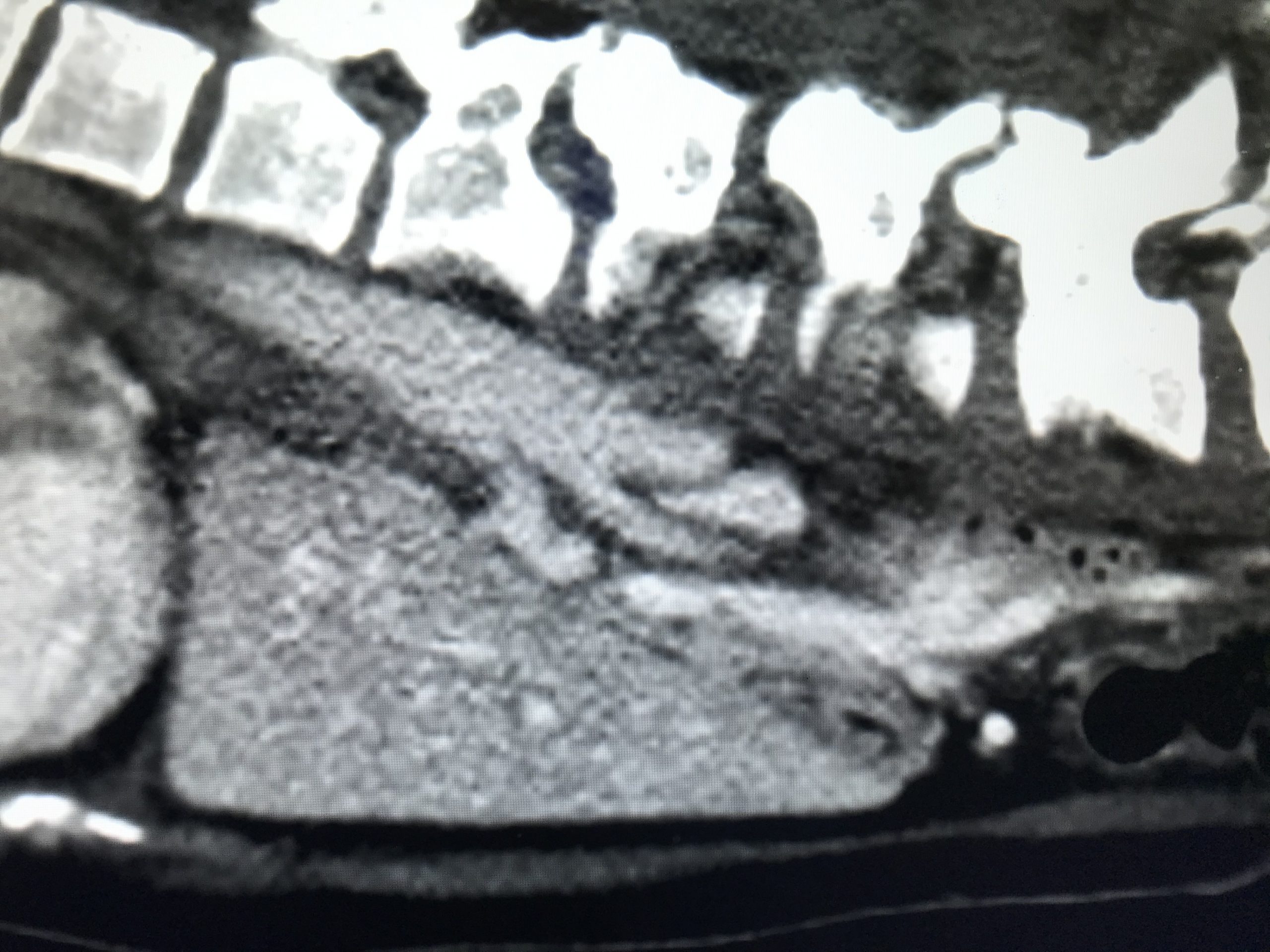
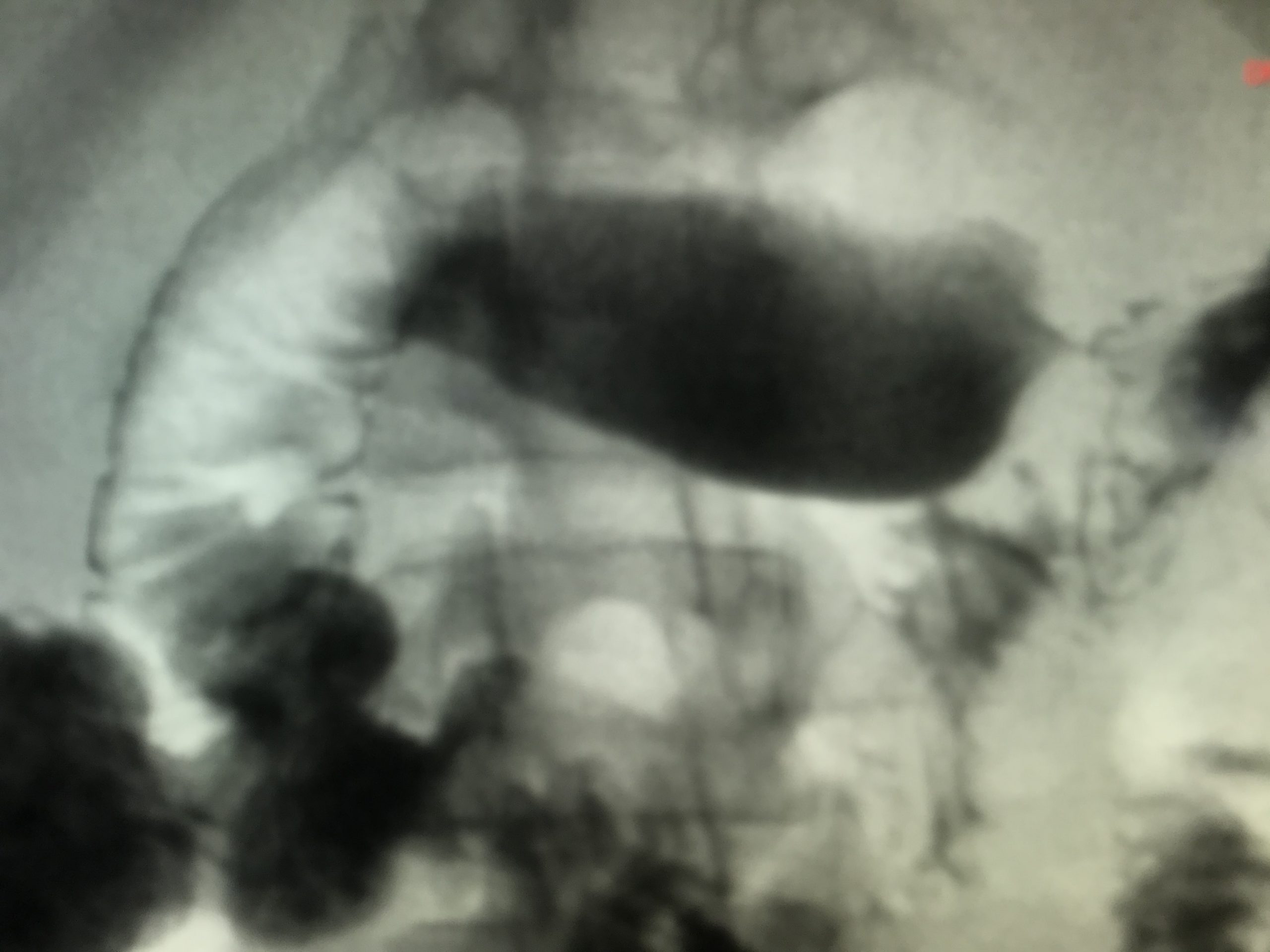
Case Presentation: 29-year-old female with a history of cervical cancer status post cervix removal in 2014 and epilepsy presented to the emergency department with a three-month history of chronic generalized abdominal pain, failure to thrive, 40 lb. unintentional weight loss and anorexia that had acutely worsened in the previous two weeks. One day prior to presentation, the patient had a witnessed generalized tonic clonic seizure that brought her to Emergency department. Upon presentation to the ED, the patient’s blood pressure was 122/77, heart rate was 77, temperature was 98 F, and oxygen saturation was 100% on room air. Laboratory studies were within normal limits. CT Abdomen and Pelvis showed no acute intra-abdominal or pelvic finding. CT head without contrast was unremarkable. The patient was administered anti-emetics and oral pain medication with little relief and was subsequently admitted to the medicine service. Gastroenterology (GI) was consulted. They had a low suspicion for malignancy, despite recent unintentional weight loss and recent cancer history because of negative imaging. GI suspected Peptic Ulcer Disease given the location of abdominal pain and history of NSAIDS use. Upper endoscopy was performed which showed a normal esophagus, stomach, and duodenum. The etiology of the patient’s abdominal pain could not be explained. The leading diagnosis was now functional abdominal pain. The patient was started on amitriptyline 25mg and omeprazole daily. Abdominal symptoms continued to persist despite all the therapies. Patient had a repeat CT scan of abdomen and pelvis, which showed that the left renal vein was compressed by the Superior Mesenteric Artery (SMA) and 15 degree angle between abdominal aorta (AA) and SMA , concerning for SMA syndrome. An upper GI series was inconclusive due to patient inability to swallow the barium. A repeat upper GI series showed dilation of the proximal duodenum relative to the distal duodenum suggestive of SMA syndrome. A gastric empty study showed normal gastric motility. The patient was offered the option of GJ-Tube placement as her main source of nutrition in order to gain weight as an initial treatment for her SMA syndrome. Patient underwent GJ tube placement by interventional radiology and tube feeding was started
Discussion: SMA syndrome is a rare digestive condition that occurs when the duodenum is compressed between two arteries (the AA and the SMA). This compression causes partial or complete blockage of the duodenum. It is potentially life-threatening and is typically caused by an angle of 6°–25° between the AA and the SMA, in comparison to the normal range of 38°–56°, due to a lack of retroperitoneal and mesenteric fat. Patient may be in a downward spiral as weight loss worsens. It can be difficult to diagnose due to non-specific presenting symptoms, including nausea, vomiting, bloating, anorexia, abdominal “crampy” pain, etc. CT of abdomen with intravenous contrast and upper GI series are required to make a diagnosis. Other GI conditions should be ruled out before a diagnosis of SMA syndrome is established. Initial treatment usually is to optimize nutrition. If symptoms persist after nutritional optimization, surgical intervention may be indicated.
Conclusions: Here we are reporting a case of SMA syndrome which could impose a challenge in diagnosis and management for hospitalists. A high clinical suspicion and prompt work up are required to make a diagnosis. Prognosis depends on whether the condition is diagnosed early and treated in an appropriate manner.