Case Presentation: Papillary fibroelastomas are among the most common primary cardiac tumors, yet primary cardiac tumors overall remain exceedingly rare, making them an uncommon source of embolization. Although most reports describe cerebrovascular presentations such as stroke or transient ischemic attack TIA¹, papillary fibroelastomas can also cause coronary embolization. We present a rare case in which a mitral valve papillary fibroelastoma was the likely source of myocardial infarction.
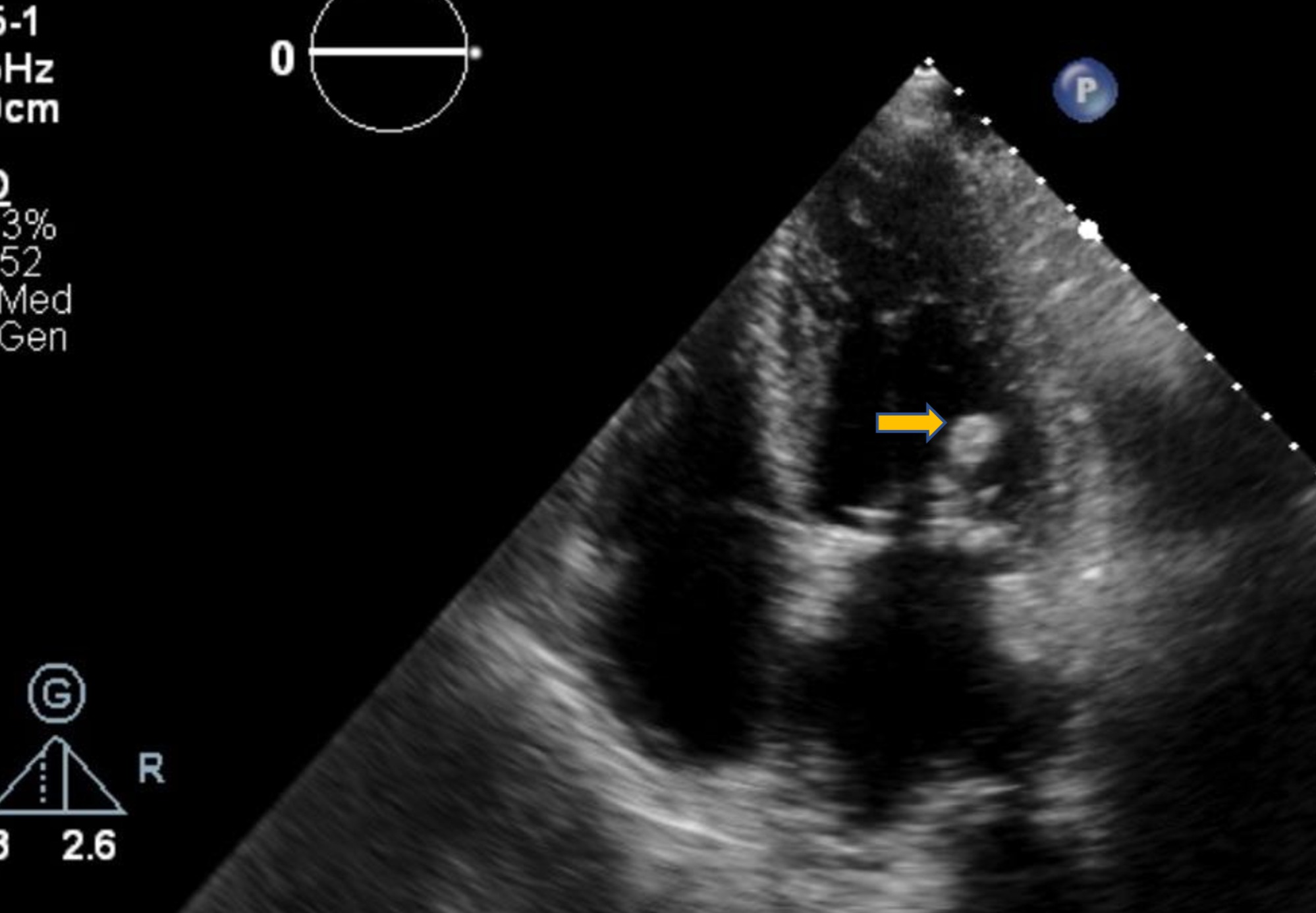
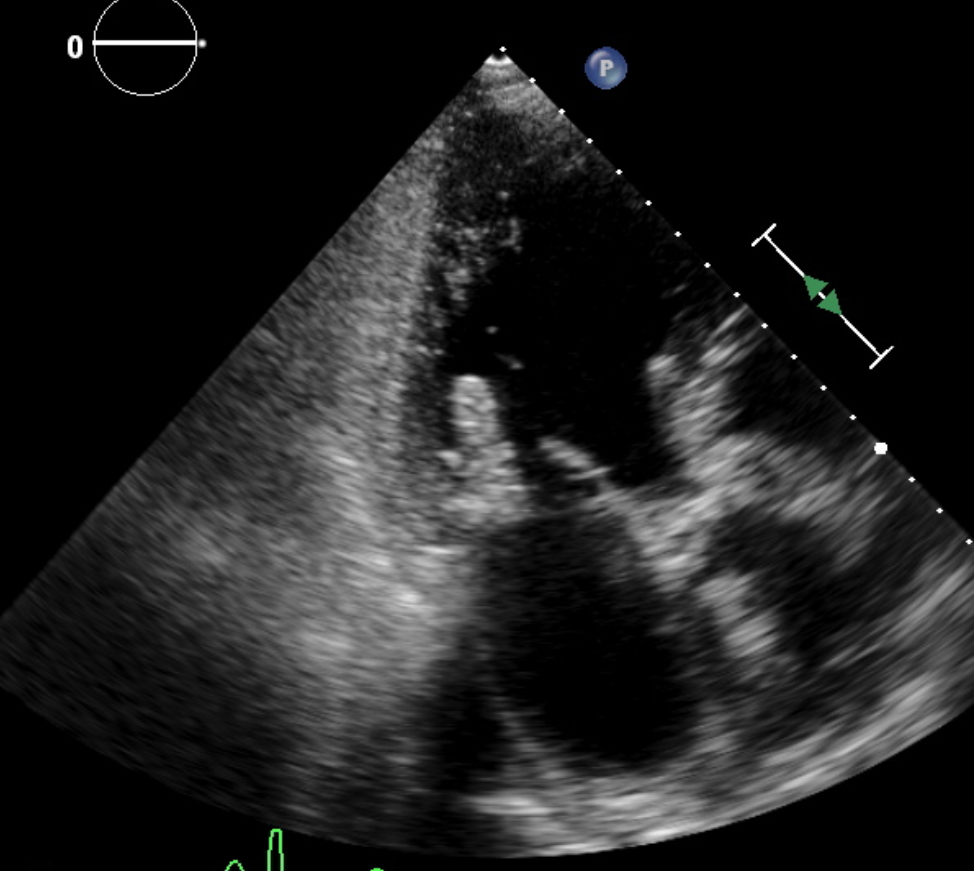
Discussion: A 64-year-old male presented to the emergency department with complaints of chest pressure lasting 3 hours at rest, associated with acute shortness of breath. Initial blood pressure was 226/112. Pertinent lab findings showed a troponin increased from 200s to 2700s and a BNP of 3500s. EKG showed non-specific ST-segment and T wave changes. The patient was admitted for NSTEMI. Left heart catheterization revealed nonobstructive coronary artery disease. Transthoracic echocardiogram revealed an incidental finding of a hyperechoic mass on the mitral valve. This prompted further investigation, and a transesophageal echocardiogram revealed more than one mobile mass on the posterior leaflet of the mitral valve in the left ventricle concerning papillary fibroelastoma. The patient was empirically started on anticoagulation with Eliquis. The patient eventually underwent cardiac MRI for characterization of the mass, and it was consistent with papillary fibroelastoma. The patient was subsequently evaluated by cardiothoracic surgery for elective surgical resection.
Conclusions: Papillary fibroelastomas are rare, but they can cause embolization, leading to myocardial infarctions, strokes, or TIAs. An echocardiogram helps identify these cardiac tumors, but the definitive diagnostic tool is surgical pathology. The mainstay of treatment for symptomatic papillary fibroelastomas is surgical resection. However, poor surgical candidates and patients awaiting cardiac surgery are at increased risk of clot formation and embolization. This case demonstrates the importance of initiating anticoagulation without any delay in preventing future MI or stroke risk events.