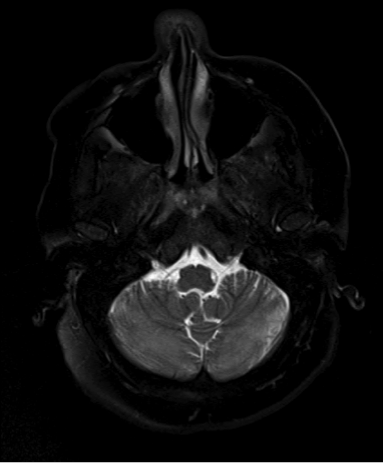
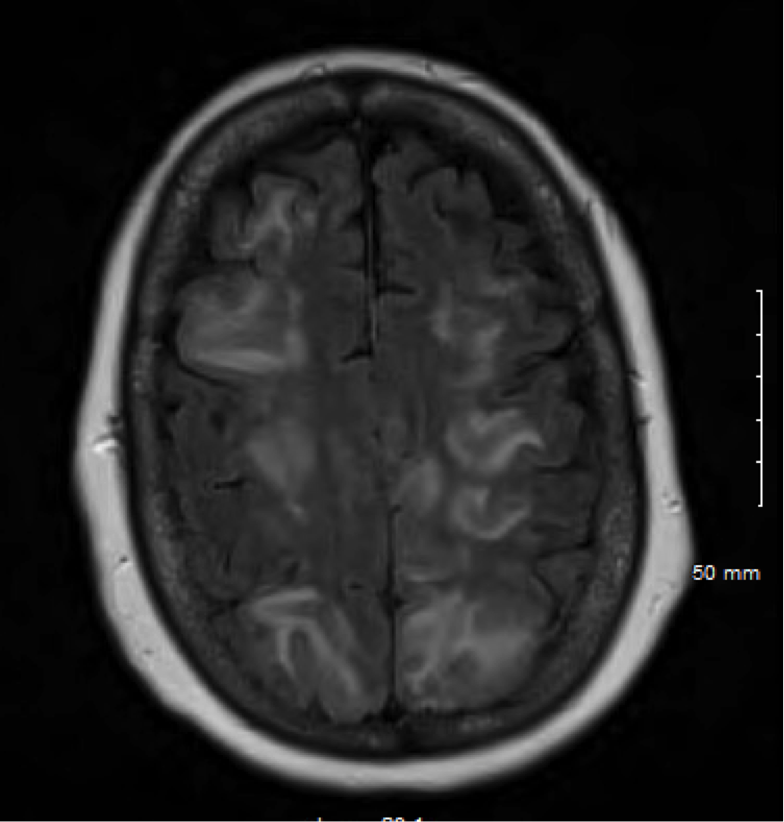
Case Presentation: A 60 year-old women with hypertension, coronary artery disease, COPD and gastroesophageal reflux, presented with one-day history of fever, witnessed tonic clonic seizure, confusion and lethargy. She reported headache for a month with back pain. Vital signs revealed fever 40 °C, tachycardia 128/min, tachypnea 32/min, and oxygen saturation of 100% on 2 L of oxygen. Exam revealed expressive aphasia and positive upper extremities cerebellar sign. Rest of neurological and cardiovascular exam was normal. Laboratory values showed leukocytes (WBC) 6.3 x10(3)/mcL, hemoglobin 14 g/dL, platelets 246 x10(3)/ mcL, sodium 138 mmol/L, creatinine 1.01 g/dL, calcium 9.3 mg/dL. Serum Lyme, syphilis, and HIV serology were negative. Serum cryptococcal antigen and EBV PCR were negative. Serum herpes simplex (HSV) 1,2 IgG was positive. MRI revealed abnormal FLAIR and T2-weighted signal in each cerebral and cerebellar spheres and brainstem (image 1, 2). Spine MRI was negative for infection. The patient was started on intravenous ceftriaxone, vancomycin and acyclovir, with significant improvement in mental status, without recurrence of fever or seizure. Lumbar puncture later showed normal cerebrospinal fluid (CSF) findings except elevated protein 144 mg/dL (WBC 0/mcL, red blood cell 3/mcL, and glucose 63 mg/dL). CSF Cryptococcus antigen, VDRL, Lyme index, HSV PCR, and VZV PCR, all were negative. Antibiotics were deescalated to acyclovir only given high suspicion of herpes simplex or varicella zoster infection, especially after detailed skin exam revealed healing gluteal rash suggestive of such diagnosis. CSF was sent for extensive panel and was positive for HSV 2 IgG and coxsackievirus B5 antibodies. Clinically the diagnosis was consistent with HSV encephalitis.
Discussion: Encephalitis was suspected given the fever, headache, seizure, and confusion, in addition to impaired brain function on exam (aphasia, cerebellar symptoms). The clinical picture was suggestive of HSV encephalitis especially with the presence of rash, however the MRI findings were not typical. HSV usually involves the temporal lobes, but a few case-reports described multifocal involvement similar to our case. Additionally, HSV PCR in CSF was negative, which could be seen in early HSV infection, but interestingly HSV IgG was positive in CSF confirming the diagnosis. Patient robust response to acyclovir treatment supported such diagnosis as well. Also Varicella zoster infection was a consideration but VZV PCR and antibodies were negative in CSF. This case is unique due to the challenges it posed with the atypical brain involvement on MRI and the negative typical studies for HSV. It also highlights the significance of detailed skin exam, which helped reaching the diagnosis.
Conclusions: HSV encephalitis is a serious infection, early diagnosis and prompt initiation of treatment is essential in management, however diagnosis could be challenging. Physicians should be aware of the rare multifocal involvement on brain MRI and the possibility of negative HSV PCR testing in CSF in early infection.