
Background:
A large majority of emergency cranial computed tomography (CCT) scans performed in the evaluation of nontrauma neurological complaints neither reveal clinically significant abnormalities nor result in emergent interventions. Over‐utilization of imaging modalities results in radiation exposure, undue reliance on imaging, delayed emergency department (ED) throughput, and increased costs. To reduce unwanted imaging, we studied the utility of focal neurological signs in identifying patients with clinically significant abnormalities on CCT who require clinically pertinent interventions such as emergency neurosurgery.
Methods:
We retrospectively audited charts of all patients between ages 18 and 89 who underwent a CCT in the ED before admission to the hospital from January 1 to December 31, 2007. We excluded patients who had any evidence of trauma, CCT at an outside hospital prior to arrival at our ED, cranial surgery, or clinically significant abnormality in the preceding 6 weeks and if they had a lumbar puncture in the ED. Demographics, chief complaint, neurological exam, results of CCT, neurosurgical interventions, and discharge diagnoses were recorded. The following were considered clinically significant abnormalities: ischemic stroke, intracranial hemorrhage, mass, infection, cerebral edema, hydrocephalus, or a combination of these findings.
Results:
In the study period, 766 patients met the inclusion criteria. As shown in Table 1, CCT revealed clinically significant abnormalities in 61 of 766 cases (8%), 45 of whom had focal neurological findings (6%). Focal neurological signs were also present in 38 patients without CCT abnormalities (false positives). Eleven of 766 patients (1%) underwent a neurosurgical intervention, only 6 (0.8%) of which were emergency procedures, all of whom had focal neurological signs (100%). The negative predictive value (NPV) of focal neurological signs is 100% for clinically significant abnormalities that require emergent neurosurgical interventions (Table 2). The sensitivity and NPV of focal neurological signs in predicting the need for any neurosurgery is also high.
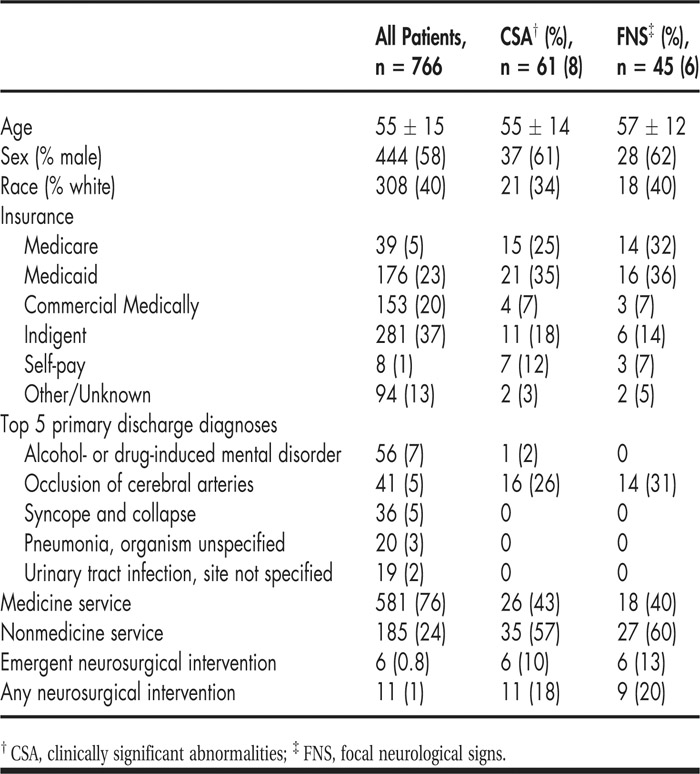
TABLE 1 Demographics

TABLE 2 Comparison of the Diagnostic Yield of CCT to Focal Neurological Signs
Conclusions:
Among nontrauma cases, the prevalence of clinically significant abnormalities and emergency neurosurgery are both low. If we restricted CCT ordering only to those patients with focal neurological signs, 643 such scans could have been avoided without missing any patient who would have required emergent neurosurgery. In the absence of focal neurological findings, emergency CCT may be entirely avoided or safely delayed based on clinical course.
Disclosures:
V. Narayanan ‐ none; A. Keniston ‐ none; R. K. Albert ‐ none