Background: At Barnes-Jewish Hospital/Washington University residency programs, non-internal medicine interns undergo a significant portion of their training via the Hospitalist Medicine Division to fulfill their ACGME requirement of inpatient internal medicine. The hospitalist schedule is a 7-on and 7-off rotation, resulting in new attendings each week for both supervising direct patient care and leading intern report. This format does not control for education consistency, ensure core internal medicine topics have been reviewed, or confirm whether educational objectives have been achieved. Furthermore, changes to the current format must allow for the most efficient use of time possible as the Hospitalist curriculum can only cover 6 hours’ worth of in-person didactic education within a given 4-week block due to the professional demands of the attendings and the inherent nature of the Hospitalist schedule.
Purpose: Our aim in this project was to create consistency within the curriculum for non-internal medicine interns by developing a combination of asynchronous and active learning curriculum that covers 8 core internal medicine topics using academic half-days (AHDs) to allow for most efficient use of time. The asynchronous portions include independent review of online learning modules and EBM journal articles which are curtailed to the intern’s rotation. The active learning portion allows for in-person discussion and review and assessment of the asynchronous assignments, and then is followed by a preset, attending-led case report presentation.
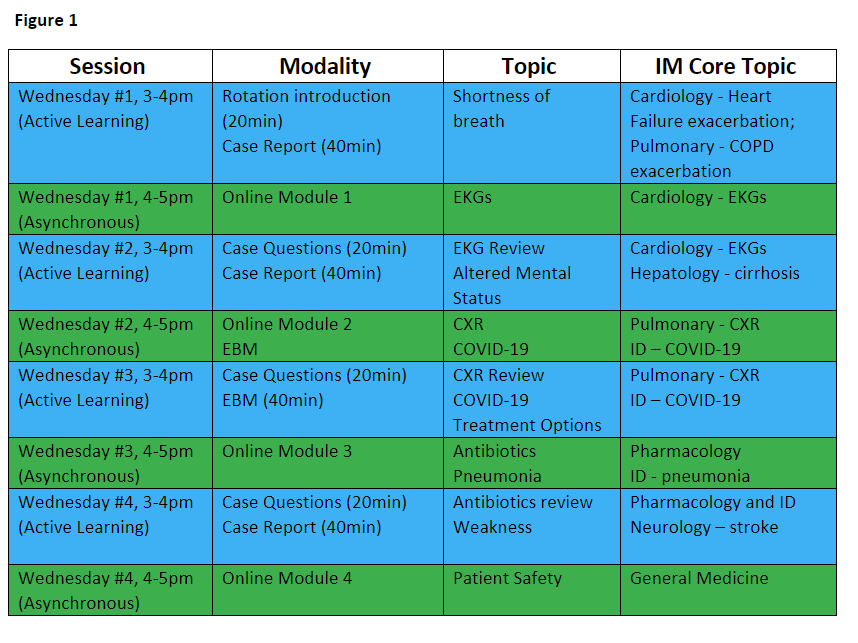
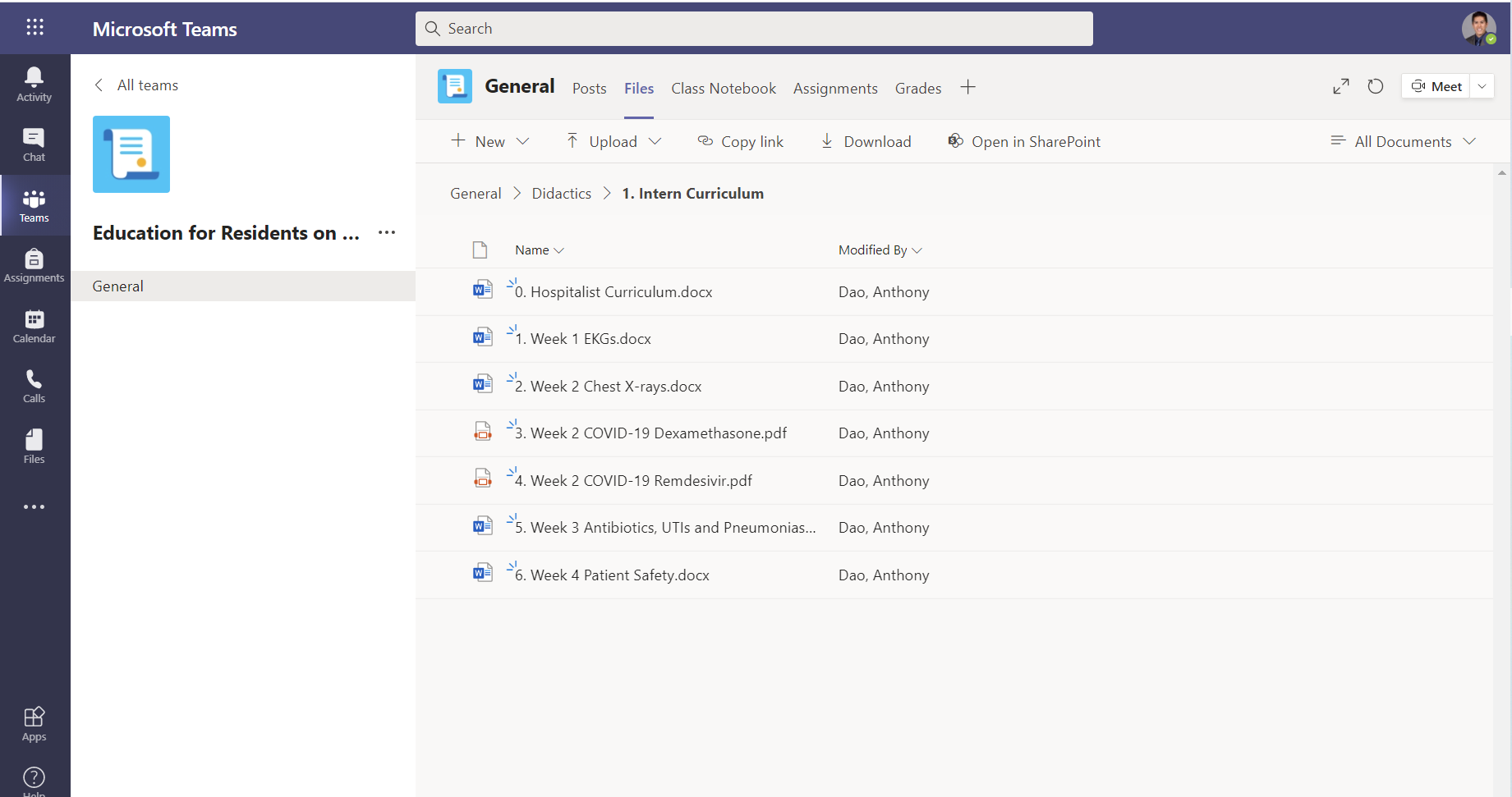
Description: There is ample evidence that protected AHDs improves learner and teacher satisfaction while also decreasing interruptions. Wednesday afternoons from 3-5pm were chosen for our AHD so as not to overlap with division grand rounds and division conferences. Additionally, this time block was felt to cause the least interference with real-time patient care. Interns are expected to complete their clinical duties by 2:45pm so they can participate in the active learning session from 3-4pm followed by an independent learning session from 4-5pm. Over a given 4-week block, the adoption of AHDs can now cover eight hours’ worth of education (Figure 1). The eight core internal medicine topics were chosen by the Resident Director and Student Director in the Hospitalist Division. Microsoft Teams, a new platform to engage both teachers and learners, was utilized to disseminate information to both attendings and learners to allow for standardized reusable content while also allowing for remote asynchronous education. The entire curriculum is uploaded to Microsoft Teams (Figure 2), and attendings and students are permitted to access all the materials at any given time to review before class. Resident, attending, and rotation evaluations were also synced to this platform to centralize the entire rotation.
Conclusions: With the implementation of a combined asynchronous and active learning curriculum, the Hospitalist Division learning objectives became finite and achievable which has allowed our division to reliably teach eight core internal medicine topics curtailed to the needs of the non-internal medicine residents. With the AHD, we also protect our faculty’s and learners’ time.