Background: There are mounting evidence that the clinical outcomes of conservative blood utilization strategy are equal or superior to liberal blood utilization in patients with anemia in the absence of severe acute hemorrhage, hemodynamic instability, or acute ischemia. However, practice variations among clinicians continue to create a challenge to effective blood utilization stewardship. Hospital Medicine at Lehigh Valley Health Network (LVHN) successfully employed a change management tool, BLOODLESS, that allowed the team to deliver significant and sustainable decrease in packed red blood cells (pRBCs) utilization well beyond the already impressive institutional achievement.
Purpose: To optimize pRBCs utilization for hemodynamically stable patients on the Hospital Medicine Service in the absence of severe acute hemorrhage or ischemia by transfusing one unit at a time and only when Hemoglobin < 7.
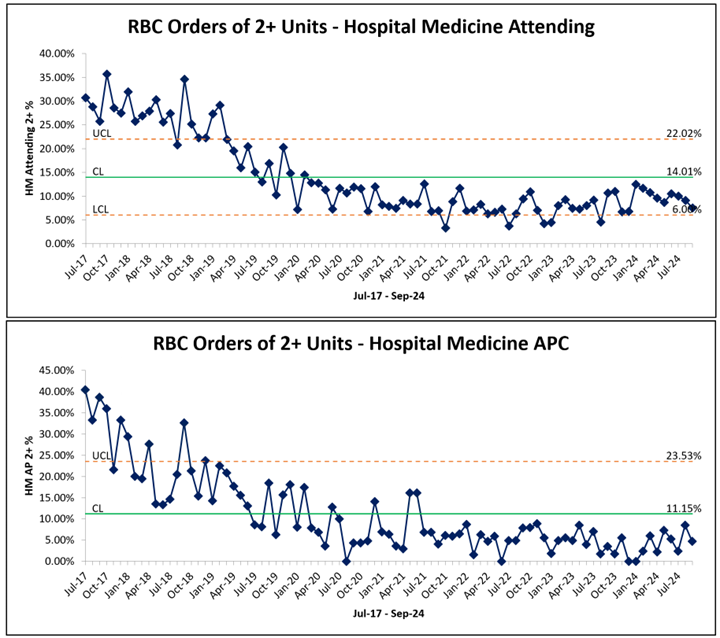
Description: Ideal blood utilization stewardship should focus on the prevention and management of anemia, optimization of hemostasis to reduce or prevent bleeding, and the promotion of optimal blood conservation with a patient-centered focus. Overutilization of blood products can be a potentially harmful intervention and certainly a costly one. Yet, blood transfusion continues to be among the most performed procedures in U.S. hospitals. Hospital Medicine at LVHN, a 15-hospitals care system in eastern PA with 327000 ED visits and 75000 acute admissions annually, employed a change management tool, “BLOODLESS” care, to supplement institutional guidelines, resources, and interventions to generate the sustainable cultural change needed to adopt a conservative blood utilization management strategy. Elements of the BLOODLESS tool include Burning platform, Literature evidence, Optimization of EMR, Operationalization of Change, Data sharing, Learnings via analysis and PDSA continuous improvement cycles, Education, Safety assurance, and Service value to all stakeholders. The patient population of focus included adults (≥18 years of age) who are being considered for blood transfusion. Excluded were patients with emergent bleeding requiring massive transfusion, patients with hemodynamic instability, or perioperative preventative measures or indications for transfusion. During the period studied (July 2017-October 2024), Hospitalists performance improved by 71.5% compared to their own historic results and outperformed the network overall results by over 55.1% (LVHN system double unit RBC orders averaged 28.7% per month vs. 12.9% by HM). A secondary outcome was significant cost saving of around $31,000 in acquisition cost per month ($375k per year) based on a conservative estimate of $205 acquisition cost per unit.
Conclusions: Hospital Medicine change management tool, BLOODLESS, has proven to be effective in driving the transformational cultural change needed to achieve a sustainable improvement in blood utilization by Hospitalists, both physicians and Advanced Practice Clinicians, for stable patients with anemia at LVHN compared to historic HM and overall LVHN performance. Similar strategy can be utilized to enact future cultural change for other QI projects that are largely dependent on behavioral alteration. As we learned in the COVID-19 era, resources could become scarce abruptly creating difficult dynamic between supply and demand, and responsible utilization is one crucial tool to navigate those challenges.