Background: There is a growing emphasis on teaching Quality Improvement (QI) to resident physicians and medical students. Successful QI training for residents and students requires faculty role models, teachers and mentors. However, faculty with QI skills and knowledge is lacking at many academic medical centers. Active learning programs to improve faculty capacity for QI have shown positive outcomes.
Purpose: To create a QI curriculum for faculty within the Division of Hospital Medicine to develop faculty capacity to serve as future QI role models.
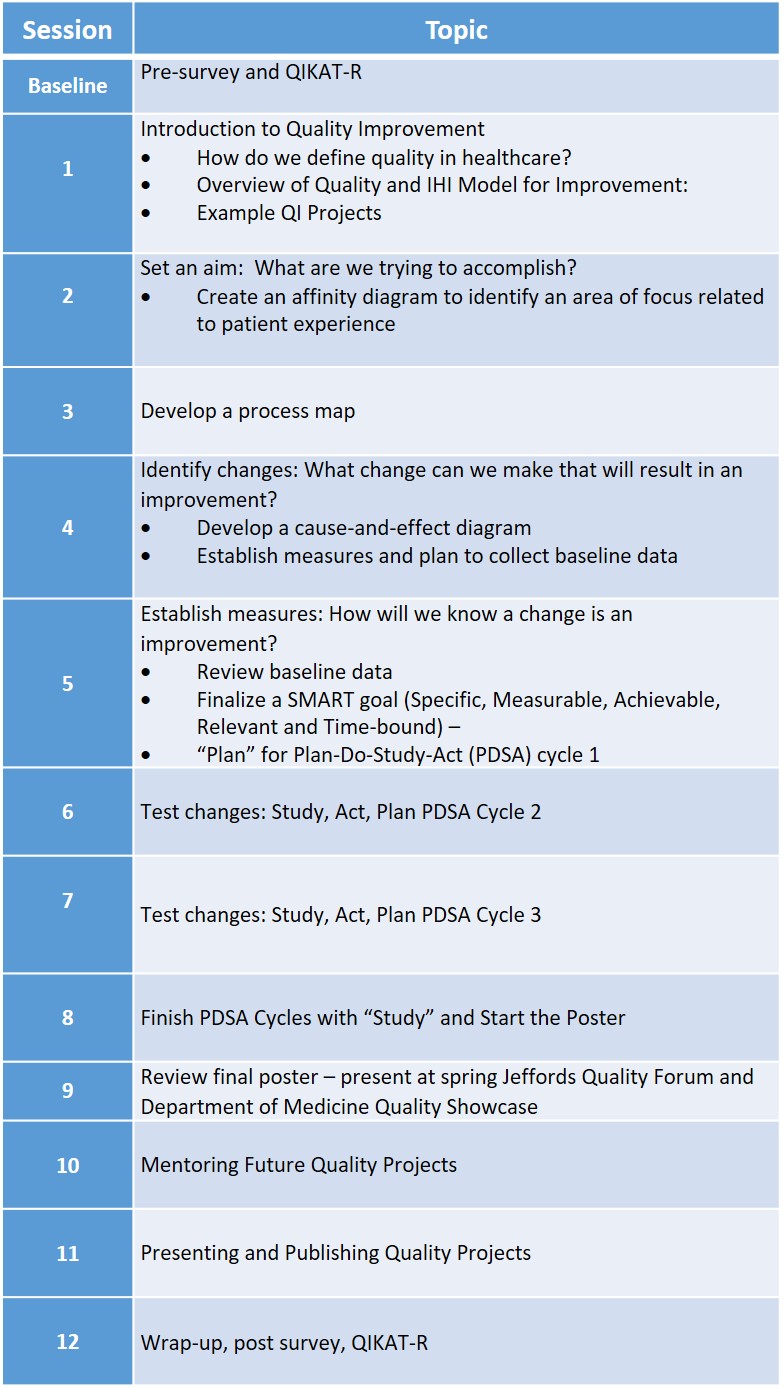
Description: Using focus group technique, we conducted a needs assessment of Hospital Medicine faculty at our academic medical center. Based on the focus group results, we designed a 12-session curriculum using an active-learning approach and incorporating core concepts in QI, an applied project, and sessions on effectively mentoring and publishing QI.(Fig) Junior and senior faculty collaborated on curricular design and delivery, with the goal of developing junior faculty into effective QI teachers. Junior faculty members were given protected time for their effort. Pre-assessment of QI knowledge, skills, and attitudes was conducted using a survey instrument and the revised Quality Improvement Knowledge Application Tool (QIKAT-R).
Six Hospital Medicine faculty members participated in the focus group. Challenges of participation due to clinical duties and goals of achieving fundamental skills in QI emerged as themes from the focus group. Eighteen faculty completed the pre-assessments (82% completion). At baseline, self-reported comfort was highest for “setting aims for a QI project” and lowest for “presenting results of a QI project”. The mean QIKAT-R score was 16.8 out of 27 (SD 4.5), with the lowest performance in the “setting aims” domain. Curricular sessions were conducted during time reserved for weekly staff meetings to minimize the interruptions to physician work flow. To date, two curricular sessions have been completed. Selected QI projects focus on improving hospitalized patients’ experiences. QI tools employed in the curriculum include affinity diagrams, process maps, and plan-do-study-act cycles.
Conclusions: We have created a QI curriculum that seeks to address the gap in QI skills among hospitalists and respond to needs identified by Hospital Medicine faculty. Pre-assessments revealed poor correlation between self-reported comfort level and QIKAT-R scores within each domain, further highlighting educational opportunities. We plan to use feedback from this pilot to refine the curriculum and offer it to faculty physicians in other specialties.