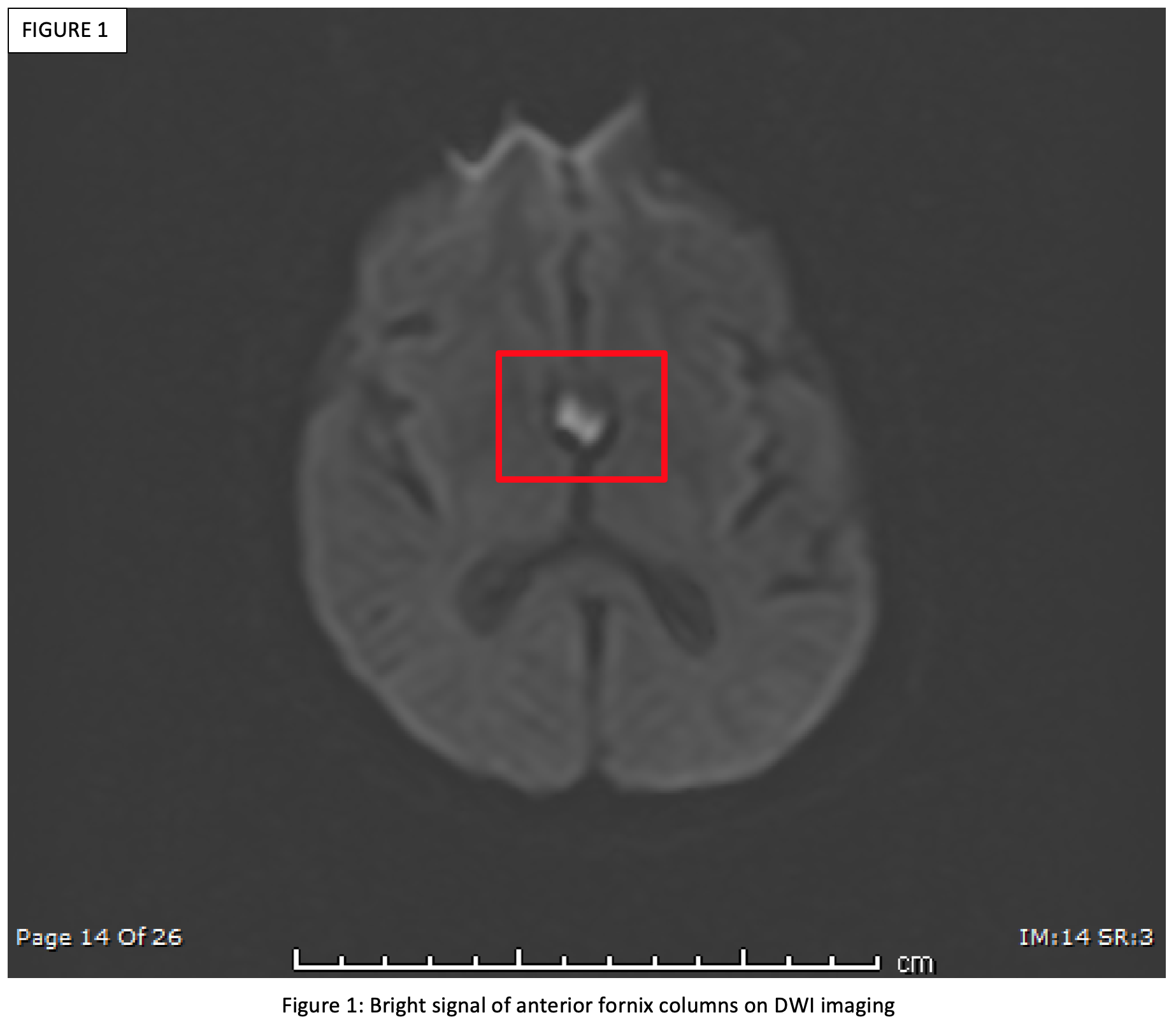
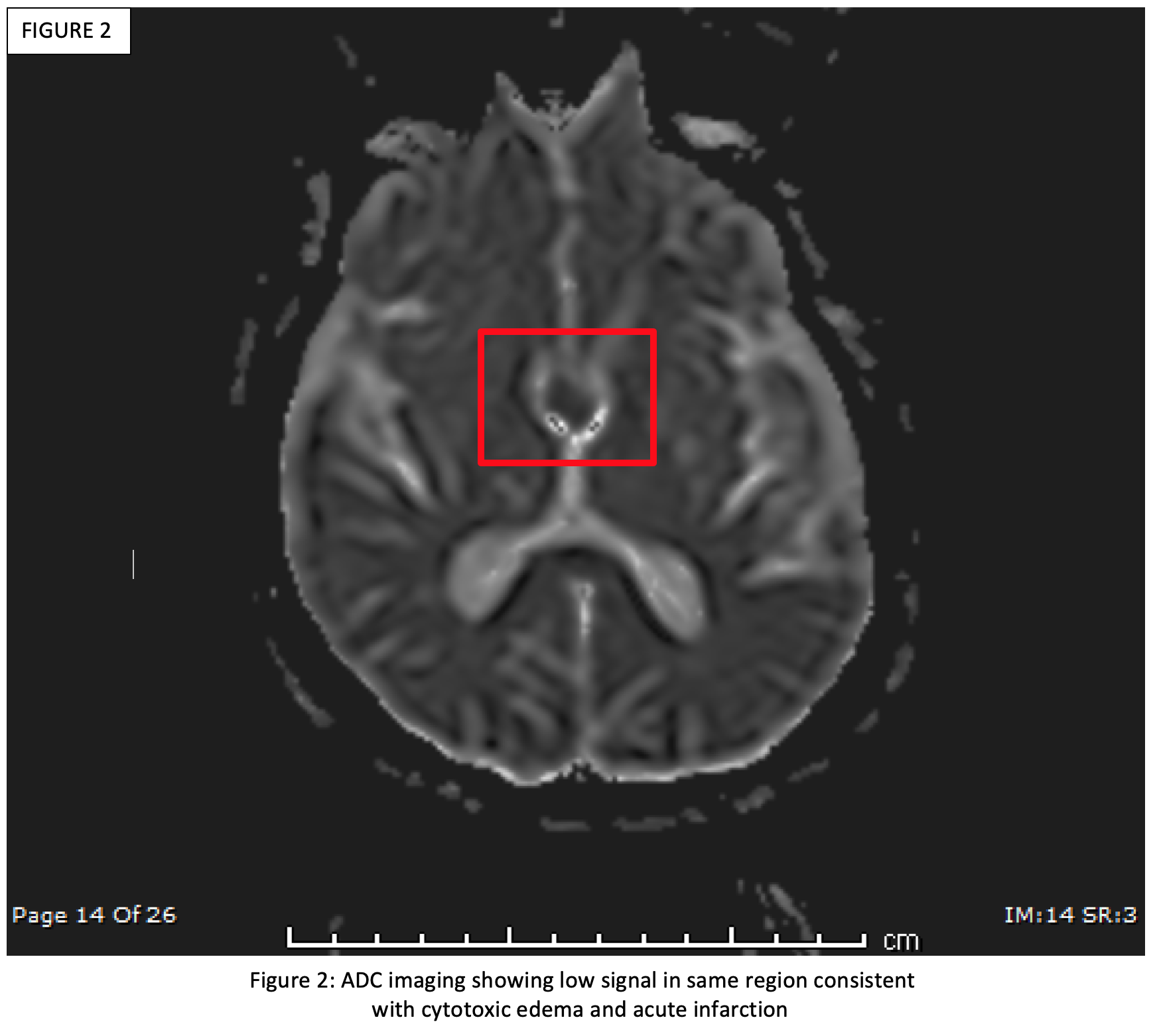
Case Presentation: 65-year-old male with chronic alcoholism, hepatitis C, prior GI bleed, and coronary disease was found unresponsive for unknown duration and was evaluated in the ED for alcohol intoxication. Patient was admitted to the hospitalist service for acute encephalopathy, acute renal failure, and alcohol withdrawal. Vital signs were stable on admission and laboratory studies were consistent with renal failure and normal hepatic synthetic function without hepatitis. Renal ultrasound, chest x-ray, and EKG were unremarkable. Head CT showed global volume loss and small superficial parietal hematoma without intracranial bleed. Physical exam showed disorganized speech consistent with delirium, orientation only to self, and no focal neurological deficits or signs of trauma.Patient was treated for alcohol withdrawal with CIWA protocol that was discontinued on hospital day (HD) 7. Renal failure resolved by HD 5. Despite resolved delirium, patient remained oriented only to self and unable to recall events since a specific day prior to admission consistent with anterograde amnesia. MRI brain on HD 7 revealed acute infarction of bilateral anterior fornix (figures 1 and 2), and appropriate treatment for acute stroke was initiated including antiplatelet agent and statins. Patient remained medically stable without further decline but no significant cognitive improvement at discharge. Patient was ambulatory and subsequently discharged home with family support. Caregiver teaching for patients with cognitive deficits was provided prior to discharge.On 2-month follow up, the patient had been started on memantine with some improvement in short-term memory. Patient requires daily reminders with whiteboard to orient to current day/time, but patient appears to be forming new memories for short duration. Per family members, patient can recall names of familiar individuals, function around the house, and able to perform activities of daily living.
Discussion: Roughly 1.2 million adults are seen yearly in acute care settings for alcohol related illnesses, of which 500,000 will require inpatient care for alcohol withdrawal and associated medical conditions. Our patient initially had altered mental status thought to be caused by alcohol withdrawal and renal failure, but subsequently found to have acute bilateral anterior fornix infarction. The identification of acute stroke in this patient was confounded by delirium, but repeat neurological exam elucidated the anterograde amnesia as delirium resolved.Infarction of the fornix and its relationship to amnesia was first described in the year 2000. The diagnosis is rare and can be missed when confounded by other causes of altered mental state associated with alcohol use. Due to the wide-ranging presentation of altered mental status linked to alcohol use, maintaining a broad differential is important if cognitive deficits remain after the resolution of delirium.
Conclusions: Anterior fornix infarction is a rare entity easily concealed by alcohol abuse, withdrawal, and many other medical conditions. In patients with acute memory changes, especially those with cardiovascular risk factors, investigation of acute stroke should be included in the initial work up so as to prevent delay to treatment.