Background: Hyperkalemia (HK; serum K+ ≥5.0mEq/L) is a common electrolyte imbalance, associated with an increase in all-cause mortality and hospitalization. Moderate to severe HK (K + levels ≥5.5mEq/L) is often managed in the emergency department or hospital, where available treatment options include methods to temporarily lower K+ (e.g., insulin-glucose and beta 2 agonists), use of cation exchange resin such as sodium polystyrene sulfonate [SPS] or initiation of acute dialysis. There is an unmet need for safe and effective therapies to rapidly restore and maintain normal serum K+. ZS-9 is a non-absorbed cation exchanger that selectively traps K+ throughout the gastrointestinal (GI) tract. In 2 large double-blind, placebo-controlled, randomized Phase 3 trials (ZS-003, and HARMONIZE), ZS-9 rapidly normalized and maintained serum K+ in HK patients. Here we present a pooled subgroup analysis of patients with K+ ≥5.5mEq/L.
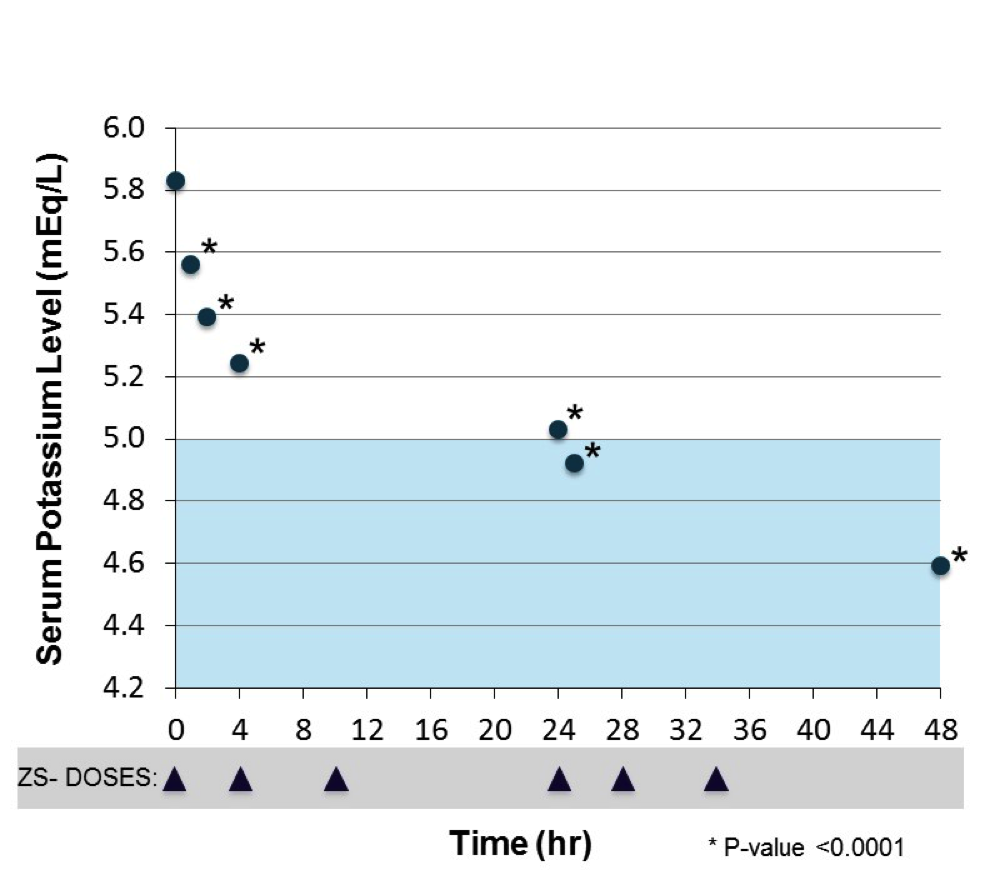
Methods: Patients received ZS-9 three times daily (TID) during a 48 hour acute phase, followed by a once daily maintenance dosing for 12 days (ZS-003) or 28 days (HARMONIZE) in an ambulatory care setting. Our pooled analysis examined 170 patients with moderate to severe HK at baseline (K+ ≥5.5mEq/L) who received 10 grams (g) of ZS-9 TID, Potassium was measured at 0, 1, 2, 4, 24, and 48 hours after the first dose. Paired t-tests were used to evaluate change from baseline.
Results: Mean K+ decreased from 5.83mEq/L at baseline to 4.59mEq/L at 48h after 10g ZS-9 with TID administration. Significant K+ reductions were observed at all time points after initial dosing (Figure; trend: p<0.0001); 72% and 95% of patients normalized by 24h and 48h, respectively. ZS-9 was generally well tolerated. In the QD maintenance phase, GI AE rates of adverse events were 3.5% for ZS-9 and 6.6% for placebo; constipation and diarrhea were most common.
Conclusions: In patients with baseline K+ ≥5.5mEq/L from two Phase 3 studies, rapid and significant lowering of serum K+ levels were observed at 1 hr after the initial ZS-9 dose. These results suggest ZS-9 is a possible non-invasive option for the acute management of patients with moderate to severe HK. Further studies with ZS-9 are warranted to determine if use of this therapy to treat HK in ED/hospitalized patients can reduce hospital admissions, length of stay and improve patient satisfaction.