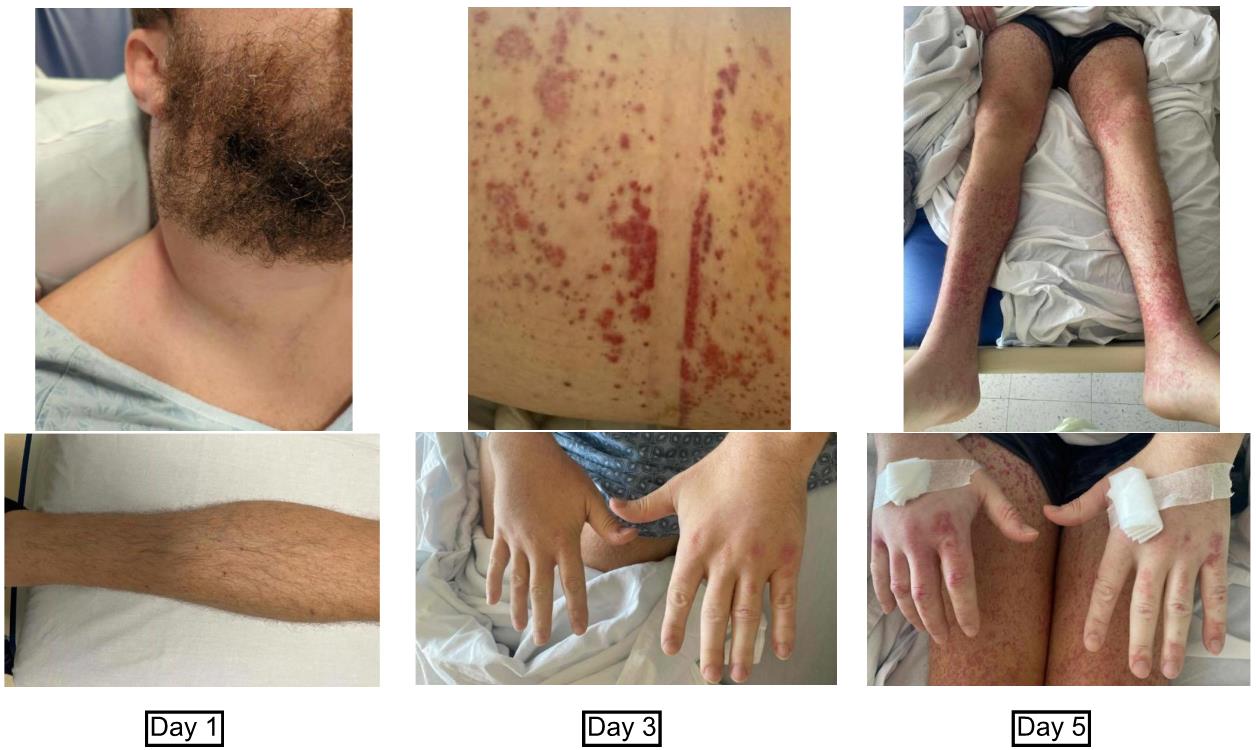
Case Presentation: A 34-year-old male without significant past medical history presented with fevers, progressive purpuric rash that started in the ankles and spread in a centrifugal distribution, joint stiffness, as well as a rapidly progressive right-sided neck mass. Two weeks prior to presentation he had experienced sore throat and subjective fevers which self-resolved. One week later, he noticed a “golf ball-sized” mass developing on his right neck. Pertinent social history included travel to Mexico 6 weeks prior and recent unprotected sexual encounters with a new male partner.Exam was notable for a large, erythematous right-sided neck mass that was tensely swollen, causing a loss of cervical range of motion and a widespread non-blanching petechial rash that was concentrated over bilateral ankles, wrists, and medial thighs, but spared the head and torso. Additionally, there was swelling and bruising of the scrotum, palms, and soles. The rash evolved and concentrated around the joints of the upper and lower extremities.Labs were notable for neutrophilic leukocytosis (17.44), elevated ESR (33) and CRP (207.2), creatinine 0.5-0.8, normal C3 and C4, and elevated IgA (658). Negative studies included HIV 1/2, Hepatitis A/B/C, syphilis, Lyme, Rocky Mountain Spotted Fever, Mumps, Parvovirus, Chlamydia, Gonorrhea, Malaria/Babesia, EBV, CMV, Erlichia/Anaplasma, Influenza A/B, RSV, and blood cultures.CT of the neck revealed bulky adenopathy with at least one necrotic lymph node and enlargement of the sternocleidomastoid muscle consistent with intramuscular hemorrhage.Fine needle aspiration and biopsy of the neck mass revealed infection with beta-hemolytic Group A streptococci. Dermatology determined his presentation was most consistent with Henoch-Schönlein purpura. He was treated with a 14-day course of amoxicillin-clavulanic acid. At outpatient follow up, his rash had resolved, and lymphadenopathy and swelling were improving. His renal function continued to be unimpaired.
Discussion: Henoch-Schönlein purpura is a clinical diagnosis based on the presence of petechiae or purpura in addition to at least one other clinical feature of arthralgia or arthritis, abdominal pain, renal dysfunction, or proliferative glomerulonephritis or leukocytoclastic vasculitis with predominant deposition of IgA on histology.1Although HSP is commonly found in the pediatric population (90% of cases), it should be considered in adults especially in the setting of recent infection, particularly streptococcal.3 The petechiae and purpura in HSP are often concentrated in areas exposed to pressure.2 This is consistent with the findings in this patient whose rash was predominantly around the joints. HSP is a self-limited disease and typically resolves within one month.2 Treatment is primarily supportive, but if streptococcal infection is identified then antibiotic therapy is recommended. The role of steroids in management is controversial. Making the appropriate diagnosis is important for continued monitoring. Within 4 weeks of initial presentation, up to 85% of patients with HSP can be found to have renal dysfunction. It is recommended that follow up include urinalysis testing each month for the first 6 months after diagnosis.2 Having a prior episode of HSP also increases the likelihood of subsequent episodes.
Conclusions: HSP is rarely reported in adults and may be due to under-diagnosis or misdiagnosis. This case highlights the course of HSP in an adult patient and that the disease may not include renal impairment.