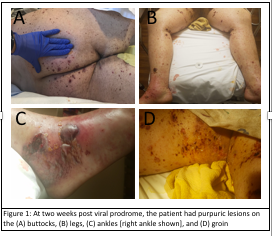
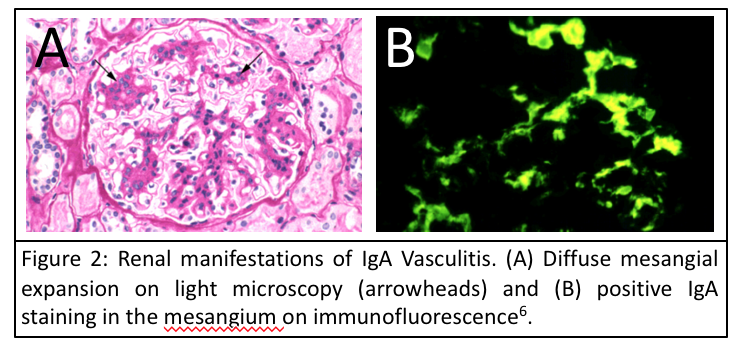
Case Presentation: IgA Vasculitis, formerly known as Henoch-Shönlein Purpura, is a systemic vasculitis most often seen in children. We present a case of a 28 yo obese man who presented to his primary care physician with complaints of fever, chills, nausea, vomiting, and sore throat for twelve hours. He was diagnosed with viral gastroenteritis and sent home with instructions for supportive care. His symptoms resolved spontaneously within two days. Two weeks later, he came to the hospital after four days of worsening purpuric rash on his upper and lower extremities that had further developed painful, open sores. Dermatology was consulted, and the patient was sent home on a prednisone taper. A skin biopsy showed evidence of IgA Vasculitis. The patient returned to the hospital two days later with worsening myalgias, lower extremity swelling, darkening urine, and transformation of the rash into more painful, open sores and bulla. Relevant labs included a UA remarkable for proteinuria, high RBC content; and markedly elevated ESR and CRP. Nephrology was consulted, and pulse steroids and lisinopril were initiated. A renal biopsy confirmed IgA nephropathy without crescent formation. After four days of hospitalization, the sores began to heal appropriately, and the patient was transferred to inpatient rehabilitation where he continued to recover.
Discussion: IgA Vasculitis is a systemic vasculitis that affects mostly children with an estimated incidence of 20 per 10,000, with peak incidence between ages four and six years old. The adult form is rare, and patients with the disease are at greater risk for developing severe complications, especially end-stage renal disease. IgA Vasculitis occurs primarily in winter months when upper respiratory infections (URIs) are at highest incidence, and nearly half of cases are associated with a recent URI with Streptococcus etiology. This is a case of adult-onset IgA Vasculitis with severe dermatologic manifestations and renal involvement. The course of the disease is clearly illustrated – an infectious prodrome, an inappropriate immune response leading to vasculitis, then renal disease. Both responded to high-dose pulse glucocorticoid therapy.
Conclusions: IgG Vasculitis is rare in adults but is associated with a higher risk for serious complications. Recognition, early diagnosis, and treatment with high-dose steroids are essential to avoiding severe complications of IgA vasculitis, especially in adults.