
Background: There is evidence that physicians consider a variety of “non-medical” factors (e.g. lack of social support, barriers to access) in hospital admission decision-making out of concern for patient safety, and that patients are hospitalized even in the absence of a level of medical acuity warranting admission. The rationale underlying this decision may overvalue the safety of hospitalization based on an assumption that patients admitted without significant medical acuity are not subjected to the same risks as acutely medically ill patients. To our knowledge, this question has not been directly investigated. Our study sought to quantify adverse events experienced by patients hospitalized without definite medical acuity in comparison to those who had a definitely medically appropriate indication for admission.
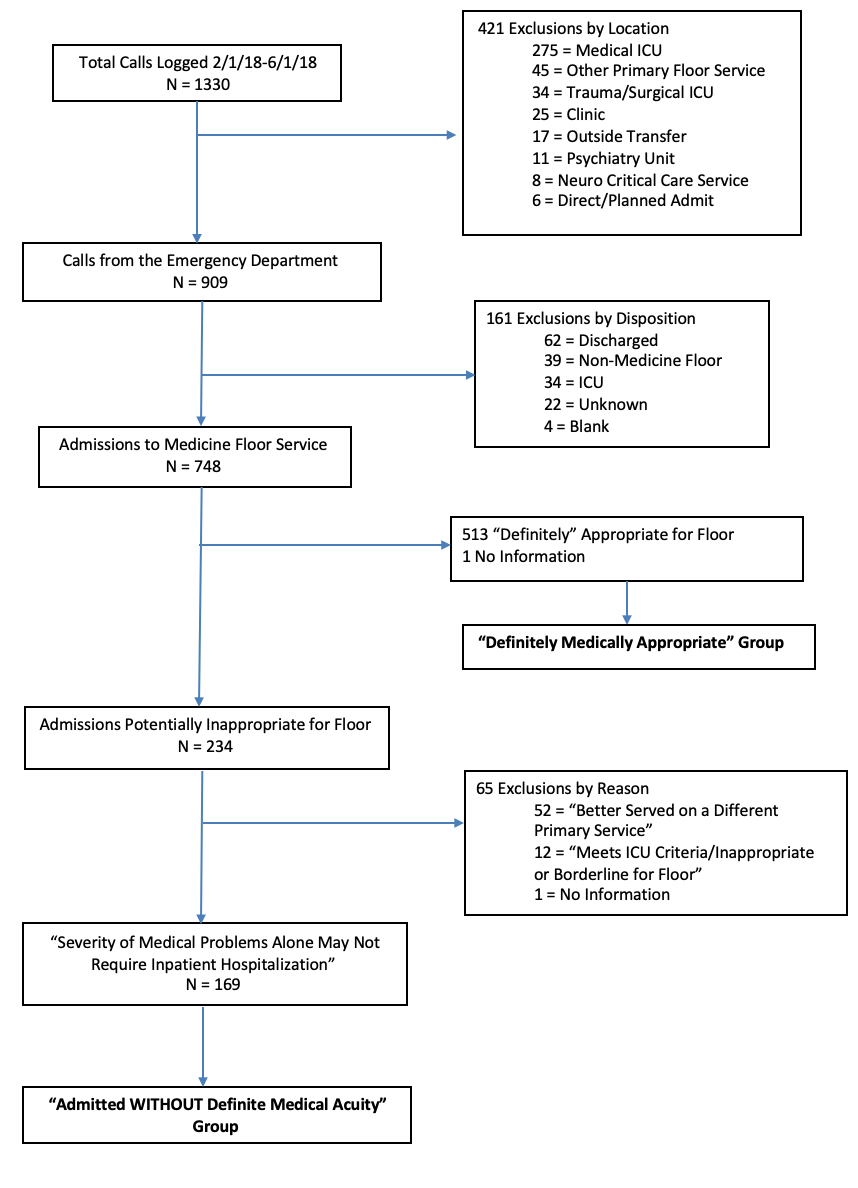
Methods: This was a retrospective cohort study of 300 admissions from 2/1/2018 to 6/1/2018 in an urban academic medical center (see Figure 1). We defined the exposure as hospitalization without definite medical acuity, as assessed by an attending physician faculty member upon admission. Chart review using the Institute for Healthcare Improvement Global Trigger tool method was used to measure adverse events. University of Washington IRB approval was granted for this study.
Results: 748 admissions from the Emergency Department to a general medical floor were included, of which 513 (68.8%) were considered definitely appropriate and 169 (22.6%) were without definite medical acuity. A sample of 150 admissions from each was used to generate cohort groups. No statistically significant differences were observed between groups in terms of age, gender, race/ethnicity, or primary language. Patients admitted without definite medical acuity were more likely to have government insurance coverage (78.9% vs. 69.8%, p=0.01), discharge to homelessness (34.8% vs. 22.6%, p=0.04), and have a longer length-of-stay (6.6 days vs. 6.0 days, p=0.038). There was no difference in the percentage of admissions with adverse events between the two groups (27.3% vs. 29.3%; RR 0.93, 95% CI 0.65-1.34, p=0.70) nor in adverse events per 1000-patient days (76.8 vs. 70.4; IRR = 1.09, 95% CI 0.77-1.55, p=0.61). The distribution of severity of adverse events was also similar between both groups (see Table 1).
Conclusions: Our findings demonstrate that patients who are admitted without definite medical acuity are exposed to the same risk of experiencing an adverse event as those who have a definitely appropriate indication for admission. Further study into the underlying reasons for these admissions and refinement of the risks/benefits surrounding the decision to admit is warranted.
.png)